





We’re now up to the final topic in the series reviewing experiences on the diet. Our final topic is the issue of weight gain and loss. This will take a few posts to explore. Next week will be “fat loss week.” This week, let’s look at the question of water weight.
Overweight people who come to the Perfect Health Diet from a high-carb diet seem to lose weight from the beginning. Here is a recent comment from Robert:
I started PHD a few weeks ago, after finding the blog, and then reading the book. I have only positive experiences to report…. I had been overweight in the past, and lost weight by low-calorie dieting on processed foods, along with strength training. After a while I would revert to some degree of overeating, and have to diet again. I’m mildly overweight now but I have been losing 2 lbs. per week on the PHD. Keep in mind this is before any calorie counting. I keep telling myself I will plug things in to Fitday, but so far my hunger is autoregulating itself and the weight is coming off.
However, some of our readers who came from very low-carb diets experienced immediate weight gains. One commenter on Amazon seemed to think this experience would be universal:
[I]f you are coming to the diet from a zero-carb or very-low-carb regimen, you can count on an immediate and substantial weight gain if you suddenly adopt the recommended intake of “400 carb calories [100 grams] per day of starchy tubers, rice, fruit, and berries.” (K. Hix)
Commenter Maggy reported a gain of 5 pounds in her first week:
Following your advice, I added back a bit of “safe starch” last week, and decreased protein intake, keeping sat fat and MCF pretty high. Well, I got on the scale today and have managed to put on 5 pounds! I’m trying to figure out what is going on and what I need to tweak. I do need to lose a good 20-30 lbs, and while I don’t want to compromise health, I also don’t want to put back on what I managed to lose doing a VLC diet.
Is this an adjustment period I need to get through? Maybe I’m one of those broken metabolism folks who has to stick with VLC?
Commenter Bill also experienced a quick gain of a few pounds, and wondered if it could be due to water weight:
After experimenting with adding modest amounts of “safe starches” to my much lower-carb routine, I have noticed a modest weight gain of 3-5 lbs. I wonder if it’s merely glycogen and water repletion.
Beth Mazur of WeightMaven.org agreed:
I also wouldn’t be surprised about weight gain. Presumably these folks are normally running on fairly low glycogen stores. Add some starchy carbs back, and the resulting water weight gain could be a handful of pounds presumably.
That’s an interesting question, so I thought I’d look into the matter.
Background: Glycogen, Glycoproteins, and Water Weight
Sugars are hydrophilic. If you put some water next to some sugar, the sugar will soak it up. As a result, a person’s water weight depends in part on the weight of sugars in the body. More sugars, more water, more weight.
It’s commonly stated that each gram of glycogen is associated with four grams of water; let’s take that as a general ratio for organic sugars.
A typical adult has around 500 grams of glycogen, roughly one-third in the liver and two-thirds in muscle. With associated water, this would add about 2.5 kg or 5 pounds to body weight.
But there are also several pounds of glucose in glycoproteins throughout the body:
- Mucus in the digestive tract and airways may be as much as 80% sugar by dry weight.
- The glycocalyx, a protective polysaccharide coat around cells, is primarily composed of sugars.
- Hyaluronan, glucosamine, and other compounds that enable joints to move freely have much of their weight as sugar-water associations.
These sugar-containing molecules with their associated water add a lot of weight to the body. Glycogen we’ve said accounts for as much as 5 pounds; mucus probably accounts for several pounds at least; and other glycoproteins must add at least a few pounds more.
Are Glycogen and Glycoproteins Lost on a Low-Carb Diet?
It’s commonly asserted that much of these sugar-containing molecules, and their associated water, are lost on a low-carb diet. From a review of Gary Taubes’ Why We Get Fat, linked today by CarbSane:
[B]etween 5-10lbs of weight are lost on a low-carb diet due to the mobilization of the water stored with glycogen …
I argued in my “zero-carb dangers” series that a danger of zero-carb dieting was that the body would downregulate production of glycoproteins; and that reduced production of these might be quite dangerous.
For instance, reduced production of mucus in the digestive tract might increase the risk of gastrointestinal cancers, bowel diseases, and entry of infectious pathogens through the gut.
If it’s true that low-carb diets reduce water weight by 5 to 10 pounds, there must be a substantial loss of sugar-containing molecules. This is hardly likely to be healthy. Glycoproteins are essential for good health. Indeed, the evolution of glycoproteins was a prerequisite for the evolution of multicellular life!
So I would find this kind of water-weight loss quite alarming.
Let’s look for some data to see if it actually happens.
From High-Carb Diet to Fasting
In our earlier post on fasting for migraines, commenter js290 linked to a very nice post by Ned Kock, in which he talked about the components of weight loss during starvation. Ned posted this picture, taken from a textbook [1]:
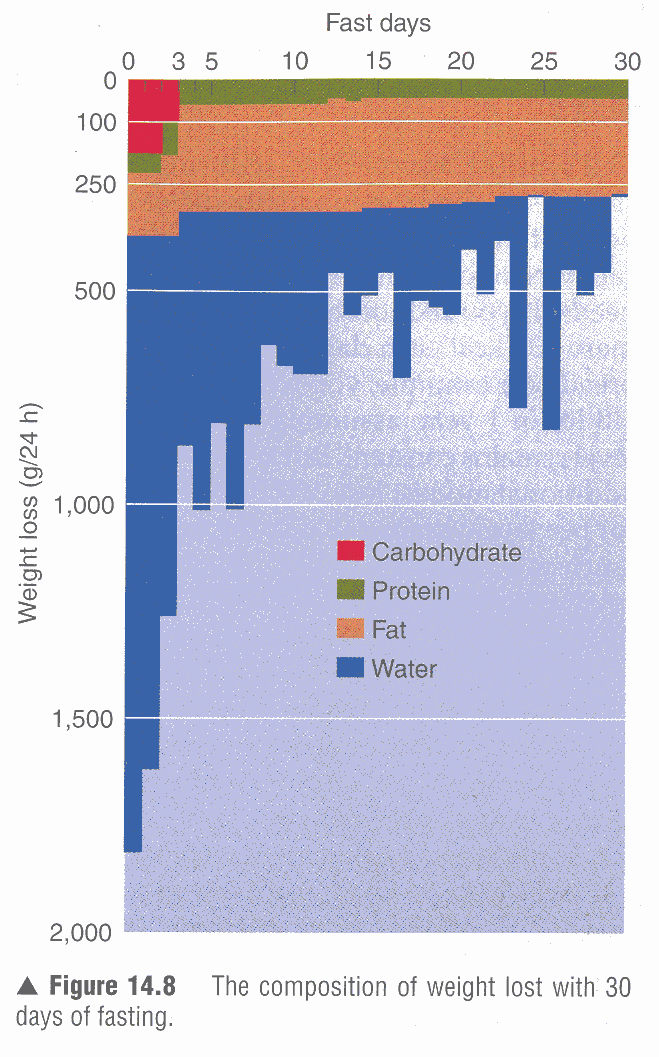
Over 30 days of fasting, almost half the weight lost is from fat and almost half from water; small amounts of protein and sugar are lost.
In the first few days, water loss dominates. In the first 48 hours, 3.4 kg are lost, of which roughly 0.35 kg are glycogen, 0.1 kg protein, 0.3 kg fat, and 2.65 kg water.
So in the first two days of fasting, fully 5.8 pounds of water are lost. That’s remarkable.
Presumably, if this person had been returned to his normal diet, that weight would have been regained in a few days.
If the water loss was triggered by a loss of carbohydrate (in glycogen and glycoproteins), then a very low-carb diet might have had the same effect as the fast.
From High-Carb to Low-Carb Diets
There are some metabolic ward studies looking at what happens when people adopt low-carb diets. Here’s one that looked at an Atkins-style diet. [2]
The subjects entered the metabolic ward but continued to eat their normal diet on days 1 through 7, to provide a baseline. Then they adopted an Atkins-style diet for 2 weeks. Carbohydrate was reduced to 21 g (80 calories) per day, and they could eat as much fat and protein as they wished.
The results:
During the low-carbohydrate diet, mean body weight decreased by 2.02 kg from 114.43 kg (last day of the usual diet) to 112.41 kg (last day of the low-carbohydrate diet) …
During the low-carbohydrate diet, mean body water decreased from 46.30 kg to 45.94 kg. Body water decreased in 6 patients, increased in 3 patients, and did not change in 1 patient. After subtraction of body water, mean body weight decreased from 68.13 kg to 66.48 kg. [2]
In other words, water weight hardly changed. The weight loss was accounted for by fat loss, which was understandable because the subjects reduced their calorie intake by 946 calories per day. [2]
So in this study, water weight loss averaged only 360 g (0.8 lb), and some patients actually gained water weight on the low-carb diet!
So it looks like going from a high-carb diet to a low-carb diet needn’t lead to much loss of water weight.
From Low-Carb Diet to Fasting
I looked for some papers on what happens when a low-carb dieter starts a fast. I found this:
In her book ‘Living on Light’, Jasmuheen tries to animate people worldwide to follow her drastic nutrition rules in order to boost their quality of life. Several deaths have been reported as a fatal consequence. A doctor of chemistry who believably claimed to have been ‘living on light’ for 2 years, except for the daily intake of up to 1.5 l of fluid containing no or almost no calories was interested in a scientific study on this phenomenon.
The 54-year-old man was subjected to a rigorous 10-day isolation study with complete absence of nutrition. During the study he obtained an unlimited amount of tea and mineral water but had no caloric intake….
[The man experienced] a mean weight loss of 0.26 kg/d … [3]
If his weight loss of 260 g/day consisted of 130 g protein and 130 g fat – a plausible mix – then he was expending about 1700 calories per day. This is very plausible, and leaves little room for water weight loss.
So when a low-carb dieter starts a fast, he may lose hardly any water weight at all!
Summary and My Own Experience
These studies are inconsistent. If going from a high-carb diet to a low-carb diet doesn’t produce water weight loss, and going from a low-carb diet to fasting doesn’t, then why would going from a high-carb diet to fasting?
I confess I was surprised by the level of water loss reported by Ned’s source. I fast moderately often, and I lose typically around 1 pound during a 36 hour fast. Shou-Ching’s experience is similar. That doesn’t leave much room for water weight loss.
But clearly, some people do experience large losses of water weight when they adopt a low-carb diet or a fast, and then regain it upon carb re-feeding.
I think we have to conclude that the phenomenon of water weight loss on low-carb diets, and water weight gain on carb re-feeding, is variable across persons. In some persons it happens, and in others it doesn’t.
Conclusion
I think those sugars serve important functional purposes. Glycoproteins are essential for health. Glycogen is a desirable reserve that helps the liver manage blood glucose and muscles exert force.
Maggy asked if she was metabolically broken because she gained 5 pounds in a week by adding carbs back in. Now, a lot can happen in a week, including significant changes in fat and protein mass, and water weight changes due to changes in sodium levels. Low-carb diets tend to lead to salt loss, so that may have been a factor.
But if the weight gain was entirely due to restoration of sugar and water levels, then I’m reluctantly led to the conclusion that Maggy may indeed be “metabolically broken.” The brokenness is not in the gain of bodily sugars when she eats the carbs; it’s in the loss of these important sugars on her very low-carb diet!
If it’s unhealthy to lose those sugars, and if a metabolically healthy person can sustain the body’s sugar and water levels through a fast, then the loss of sugars on either a low-carb diet or fast suggests a damaged metabolism.
As much as Maggy wishes to lose weight, it is important to lose weight from adipose cells, not from water and glycoproteins. Her rapid ~5 lb weight gain upon shifting from a very low-carb diet to the Perfect Health Diet might have been a very good thing.
UPDATE:
CarbSane has begun a series on water weight, and has interesting numbers on water weight in adipose tissue and lean tissue, and how water weight varies between obese and lean persons. This post introduced several papers, and a follow-up contributes an interesting analysis and suggests that movement of fatty acids between adipose and lean tissue may be involved in water weight changes.
I didn’t know that extracellular water weight in tissues was so variable. Thank you CarbSane!
References
[1] Wilmore, J.H., Costill, D.L., & Kenney, W.L. (2007). Physiology of sport and exercise. Champaign, IL: Human Kinetics. Cited by Ned Kock, “The amounts of water, carbohydrates, fat, and protein lost during a 30-day fast,” http://healthcorrelator.blogspot.com/2010/10/amounts-of-water-carbohydrates-fat-and.html.
[2] Boden G et al. Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. Ann Intern Med. 2005 Mar 15;142(6):403-11. http://pmid.us/15767618. Full text: http://www.annals.org/content/142/6/403.full.pdf.
[3] Heusser P et al. Nutrition with ‘light and water’? In strict isolation for 10 days without food – a critical case study. Forsch Komplementmed. 2008 Aug;15(4):203-9. http://pmid.us/18787329.




Recent Comments