





The Perfect Health Diet
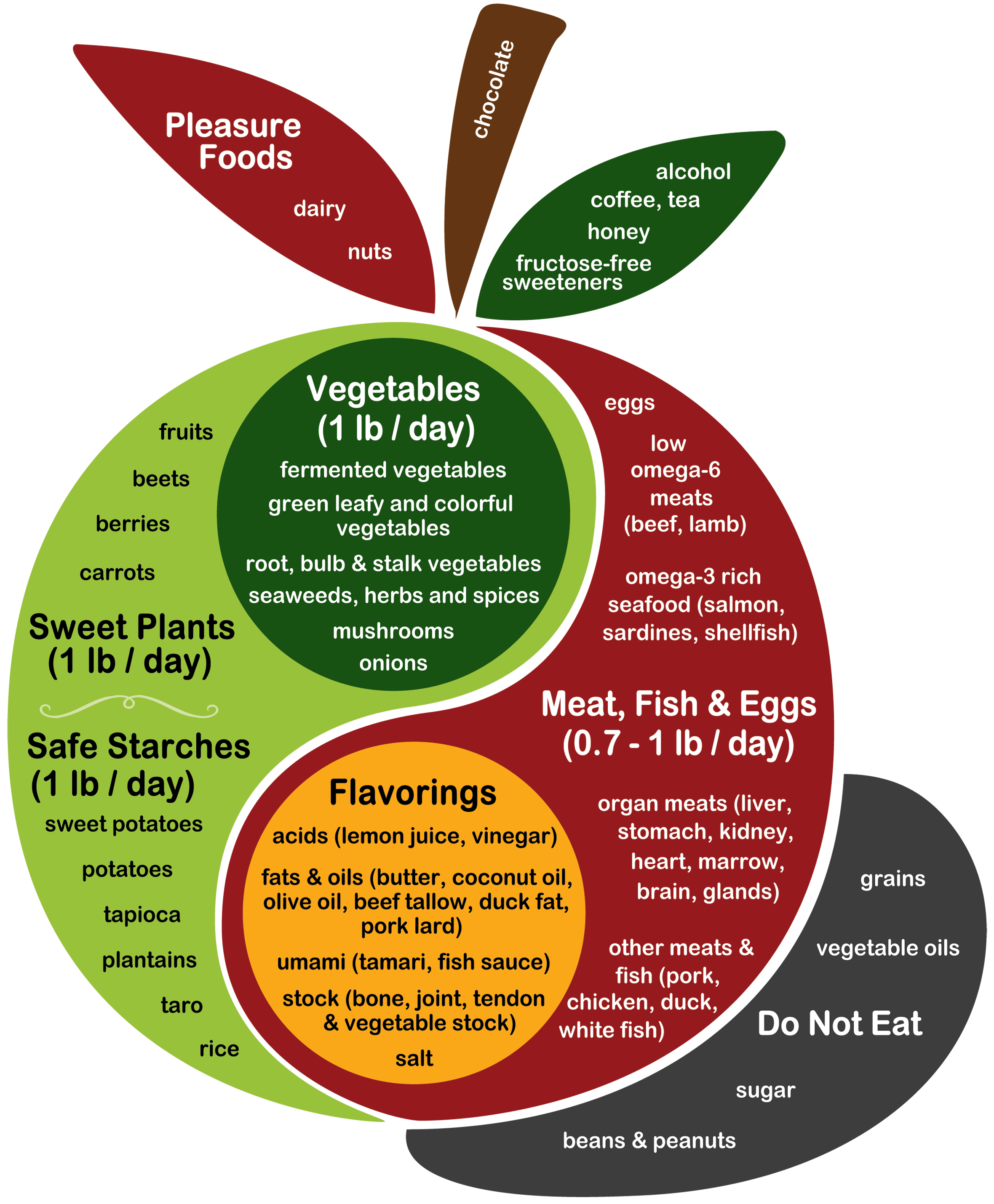
Here’s our Perfect Health Diet food plate:
NOTE: This is our new food plate, updated 2015. Foreign translations of the original food plate may be found here.
We recommend:
- About 3 pounds [1.4 kg] of plant foods per day, including:
- About 1 pound [0.45 kg] of safe starches, such as white rice, potatoes, sweet potatoes, and taro;
- About 1 pound [0.45 kg] of sugary in-ground vegetables (such as beets or carrots), fruits, and berries;
- Low-calorie vegetables to taste, including fermented vegetables and green leafy vegetables.
- One-half to one pound [0.25 to 0.5 kg] per day of meat or fish, which should include organ meats, and should be drawn primarily from:
- ruminants (beef, lamb, goat);
- birds (especially duck and wild or naturally raised birds);
- Shellfish and freshwater and marine fish.
- Low omega-6 fats and oils from animal or tropical plant sources, to taste. Good sources include:
- butter, sour cream, beef tallow, duck fat;
- coconut milk or oil
- palm oil, palm kernel oil, olive oil, avocado oil, macadamia nut butter, almond butter, cashew butter
- Acids to taste, especially citric acid (lemon juice, lime juice, orange juice, grapefruit juice), lactic acid from fermented or pickled vegetables, vinegars, tannic acids from wine, and tomatoes.
- Broths or stocks made from animal bones and joints.
- Snacks or desserts from our pleasure foods: fruits and berries, nuts, alcohol, chocolate, cream, and fructose-free sweeteners like dextrose or rice syrup.
By weight, the diet works out to about 3/4 plant foods, 1/4 animal foods. By calories, it works out to about 600 carb calories, primarily from starches; around 300 protein calories; and fats supply a majority (50-60%) of daily calories.
In the shadow of the apple are foods forbidden because of their high toxin content. Notably:
- Do not eat cereal grains — wheat, barley, oats, corn — or foods made from them — bread, pasta, breakfast cereals, oatmeal. The exception is white rice, which we count among our “safe starches.” Rice noodles, rice crackers, and the like are fine, as are gluten-free foods made from a mix of rice flour, potato starch, and tapioca starch.
- Do not eat calorie-rich legumes. Peas and green beans are fine. Soy and peanuts should be absolutely excluded. Beans might be acceptable with suitable preparation, but we recommend avoiding them.
- Do not eat foods with added sugar or high-fructose corn syrup. Do not drink anything that contains sugar: healthy drinks are water, tea, and coffee.
- Polyunsaturated fats should be a small fraction of the diet (~4% of total calories). To achieve this, do not eat seed oils such as soybean oil, corn oil, safflower oil, sunflower oil, canola oil, or the like.
We highly recommend certain foods for their micronutrients. These include liver, kidney, egg yolks, seaweeds, shellfish, fermented vegetables, and bone broths.
We also recommend augmenting the diet with certain supplements. See our Supplement Recommendations page. These nutrients are deficient in modern diets due to removal of minerals from drinking water by treatment, depletion of minerals from soil by agriculture, or modern lifestyles that deprive us of vitamin D by indoor living.
We recommend tweaking the diet for certain diseases. Neurological disorders often benefit from a diet that is ketogenic; other conditions may benefit from lower carb diets. These variations are discussed in the book:
See the “Buy the Book” page for other purchase options.




Two weeks in…added rice and potatoes back into my diet…I feel no different other than constipation + weight gain. Chronic fatigue has not changed.
I guess nobody has any suggestions or is willing to troubleshoot. ❓
Hi Rick,
You could try posting your query to the FB group… but it can be quiet there. But you never know your luck.
https://m.facebook.com/groups/476375132470281/
Thanks. I’ve actually gained 4 lbs. since I started. Was 194. Now 198. Goal is 175!
I joined it and just left it.
I prefer to deal with people whose response to a comment is a laugh emoji.
I refuse to deal with people whose response to a comment is a laugh emoji.
What is your opinion on buckwheat and quinoa on this food plate? I eat those as my primary carb sources and was considering sprouting them too
Hi Rick
I’m someone who’s suffered with many of the symptoms of chronic fatigue for years. I’m not a scientist, not even an expert, but I am a PHDer 🙂 Here’s a few points to consider:
This diet isn’t necessarily going to cure all diseases. Some people have reported major improvements or cures on the diet alone, as you might see in the testimonials, but in many cases it’s just a very valuable first step.
If you haven’t already, give the diet a good few months. I’d imagine the likelihood of noticeable improvements increases the more your current diet differs from the PHD.
Paul has posts on constipation and has recommended antioxidants for this. I assume his advice hasn’t changed so optimising zinc, selenium and vitamin C may help. Are you also eating liver, fermented foods and bone broth? Bone broth’s the best thing about PHD! So tasty – and I find it has helped gut symptoms, often immediately!
Also optimise the other supplements as per advice on supplements page – vitamin D, vitamin K, iodine and magnesium.
Hypothyroidism can constipation as well as fatigue.
Finally, chronic fatigue has been linked to chronic infections. Once you’ve optimised diet and (as far as possible) gut function, you might want to pursue that as a possibility. There are posts here about chronic bacterial infections.
Have you also read the Jaminet’s advice on circadian rhythms?
That should be “Jaminets’ advice” 😊
In addition, if you’ve been on a very low carb diet, you might want to go slowly with adding in starch to your diet as your body (and possibly gut bacteria) adjust.
Hi Rick,
I am sure that your diet is not mine and won’t be the diet of somebody else. Naturopathy is about that : you ll find YOUR way to be in health and in peace but what is sure is that we need to stop transformed food / food which is not a real one (if you put some food out of a box… Mmm it sounds bad 😉 ). And remind that coffee and tea are not food and bad for our body too. We need to limit coffee, tea + chocolate. Last but not least : milk and everything made with milk. My Best friend used to Love that but lost 8 kilos just with that. Very important to eat everything but not that 🙂 good luck !
Hi Harry, Could you guide me to the information on chronic bacterial infections? I am new to all of this and I believe this is what I have along with my autoimmune disease and chronic fatigue, chronic diarrhea. Thank you, Linda
What was your diet before? What is it now? Also, 2 weeks is not a very long time.
Hi Paul- Do you believe the COVID vaccines are safe to receive? Thanks.
Hi TR,
If by safe you mean without their own direct negative effects and without a risk of enhancing the severity of COVID, no, I don’t believe the Pfizer or Moderna mRNA vaccines are safe. There is an immediate risk (peaking about 2 weeks after each injection) of an immune attack on the vasculature or hematopoietic cells of the bone marrow, and a delayed risk of antibody-dependent enhancement of the inflammatory response to later COVID infection which could exacerbate the disease.
Whether getting vaccinated is better than not being vaccinated is an open question for which we need more data, but the vaccines are certainly not without risk, and the risk from the vaccines could outweigh a risk reduction from the disease.
The traditional inactivated virus vaccines that China is using on its population are much less risky in my view, though also not completely without risk.
Best, Paul
THANK YOU PAUL!!!! A recent post on the vaccines by Anthony Colpo gave me pause and I was very interested on your take. THANK YOU.
Hello Paul,
What does an attack on the hematopoietic bone marrow cells entail? What symptoms manifest? Is there anything we can do to minimize or prevent possible negative effects of these mrna vaccines? I’ve read about people experiencing tingling sensations in their extremities, brain zaps, vivid dreams, and even those reports of deaths within days to a couple of weeks of receiving the vaccine, a couple which made the news, for example. What could be the cause of these types of symptoms…the adjuvants? Or something to do with the mrna? What are your thoughts on ADE? Do you think enough time has passed to where we should have seen that present by now? Thank you.
Hi Yulia,
There’s nothing I’m aware of that can be done to minimize negative effects of the vaccines, apart from things that generally improve health. There are a variety of pathways by which the vaccines could cause problems, including toxic stabilized nucleotides, toxic pegylated molecules, expression of toxic viral proteins, induction of inflammatory attacks upon cells expressing the foreign protein (which is needed for the vaccines to generate immunity), induction of autoimmunity, and of course antibody-dependent enhancement of infections. ADE is a function of the coronavirus and even if ADE is not present in existing versions of COVID, it could be present in future COVID variants, that is to say, there could arise a new COVID variant which creates more serious disease in the vaccinated than the unvaccinated, even if the vaccines protect against the current version of COVID.
Best, Paul
Hi Paul and Yulia,
Any risks of vaccination must be weighed against the benefits — that vaccination essentially eliminates both risk infection and mortality from COVID, at least for the currently-circulating strains. (This is clear from the clinical trial data of the mRNA vaccines [1,2], and also from the epidemiological data from Israel [3], the first country to administer the mRNA vaccines at a wide scale.)
So how big are these benefits? The fatality rate of COVID is about 1 in 200, and the rate of serious and long-lasting complications is higher than that. Without vaccination, there is a significant chance that you will eventually be infected (probably about 1 in 3 US residents have already been infected).
Most of the risks Paul mentioned are direct adverse effects of the vaccine. There is simply no way that these direct risks could be comparable to or larger than the risk of COVID mortality/morbidity posed by remaining unvaccinated — if that were so, we would have noticed in the clinical trial data (and also in the epidemiological data). Indeed, the clinical trials of the mRNA vaccines (pooled) had about 70,000 participants. Mortality in the vaccine group was (slightly) lower than in the placebo group, and the overall mortality rate was about 1/5000 in the first two months or so. Note that this is an order of magnitude lower than the mortality rate from COVID infection (two months is short enough that only a small fraction of participants were exposed to COVID in this time frame). Beyond mortality, all of these participants were monitored closely for potential serious adverse effects, and none were discovered. So serious adverse effects must be rare. Epidemiology can give us an additional check. For example, after administering millions of doses, we had no problem noticing a 1/1000000 risk of a blood clotting disorder with the Johnson and Johnson vaccine, which was induced by the adenoviral vector. (That the FDA paused administration of the Johnson and Johnson vaccine on this basis is yet another proof of their incompetence. Can they not compare 1/1000000 and 1/200 and observe that this risk is orders of magnitude smaller than the risk of remaining unvaccinated?)
What about the risk of ADE? In other words, what if one is infected with, or vaccinated against, the current strain of COVID, resulting in non-neutralizing antibodies towards a future strain of COVID that enhance the disease? First of all, this risk is pretty speculative: ADE is the exception, rather than the rule, with most cases involving viruses like dengue fever or HIV that display significant tropism for immune cells. And no ADE has been noted with current strains of COVID. So it is rather more likely that vaccination against current strains of COVID would be neutral or protective against future strains. That said, the possibility of ADE with future strains cannot be ruled out by current data.
But even if the possibility of ADE is real, declining the vaccine does *not* eliminate the risk here — it likely *increases* it. If you remain unvaccinated, there is a significant chance you will be infected with current strains of COVID, and infection may pose a significantly greater risk of ADE than vaccination. Why? The mRNA vaccines were designed with minimization of ADE risk as a consideration. They include *only* the spike protein, and none of the other COVID proteins. So you only have one viral protein against which to make non-neutralizing antibodies, rather than many. Moreover, a priori, an antibody against the spike protein is likely to be neutralizing, because the spike protein is what binds to ACE2. So these mRNA vaccines have less potential for ADE than inactivated virus vaccines or infection. (All of this discussion, of course, ignores the question of where these future strains responsible for the ADE would be coming from: From people that have not been vaccinated, and were instead infected with current strains of COVID, thereby giving COVID a chance to mutate!)
In short, I am confident that the mRNA COVID vaccines are safe (by which I mean safer than not getting the vaccine). I got my first dose last week.
Best,
-Eric
[1] https://www.nejm.org/doi/full/10.1056/NEJMoa2034577
[2] https://www.nejm.org/doi/full/10.1056/nejmoa2035389
[3] https://www.nejm.org/doi/full/10.1056/NEJMoa2101765
P.S.: I should also point out that inactivated virus vaccines typically produce only an antibody response, without a good T cell response. This increases the chance of ADE. By contrast, the mRNA vaccines we are discussing cause the antigens to be synthesized intracellularly (as they are in an actual viral infection), and therefore *do* produce a good T cell response.
Hi Eric, Paul and Yulia,
I really appreciate this discussion and hope it is updated as the data evolves. I’m *terrified* of contracting COVID. I understand the devastation and potential long term disability it can cause even in the young and healthy. I feel the negative effects of natural COVID infection are greater than the risks of vaccines. The mRNA vaccines seem like a safer option compared to contracting COVID but I’m curious if anyone has thoughts on Novavax which uses a more traditional mechanism? Unfortunately, not yet available.
For me, I can’t see a path where not getting vaccinated is an option. This would mean I would need to go into isolation indefinitely while the rest of my family goes back into the world to live their lives vaccinated. I just cannot afford the risk of getting COVID. So then what the heck is one supposed to do then lol.
Thanks.
Hi Eric Larson,
Are you the same Eric who years ago shared a non-supplemented version of the PHD? And who also shared his literature research on the most recommended legumes and how to prepare them? Plus many other interesting contributions.
If so, do you have a blog? If you write stuff I’d love to read them.
And, is there any way to contact you? Depending on your availability, I’d love to know your thoughts on certain ideas. If you don’t have a way to be contacted that you can make public, I can leave here an email that I don’t use, so you can write me instead (and if I get SPAM from mail-tracking bots afterwards, it won’t matter).
Thanks,
Take care
Hi Alexandra,
Well, we have more data on the mRNA vaccines, which have been administered at scale. But I think the available data on Novavax looks pretty good. Note that Novavax includes a newly-designed adjuvant that promotes T cell recruitment.
I don’t see a reason to favor Novavax over the mRNA vaccines (Moderna/Pfizer). And the mRNA vaccines have the advantage that they are available now.
(I would favor the mRNA vaccines or Novavax over the Johnson&Johnson vaccine — some people will mount an immune response to the adenoviral vector used by J&J. The same goes for other vaccines based on viral vectors including AstraZeneca.)
Best,
-Eric
Hi,
Yes, I’ve written a number of comments here over the years. Both of the ones that you mentioned are mine.
No, I do not have a blog of my own.
If you think other PHD readers would be interested the discussion, why not post your questions here? If not, sure, you can leave contact info here, and I can email you (or Paul can probably put us in touch).
Best,
-Eric
Hi Eric,
I’m very happy to know that it’s you indeed. I have enjoyed your contributions on this site a lot. Some of them have had a lasting impact in my daily life, as when I prepare pulses or decide my ingredients or spices. I’m very grateful.
Yes, we can talk in private as it will be maybe more straigh-forward and less messy, but then if there is any valuable contribution we can write it here so that any person interested in PHD can access it.
You can send me an e-mail to:
zanonioideae@gmail.com
See you!
I have so many questions! I try to read studies, but I don’t feel I have the background to answer questions that come up. This is an old article in the world of covid-19 research, but I wonder if some of these concerns are still relevant or if new research has eliminated them.
“Aside from questions of safety that attend any vaccine, there are good reasons to be especially cautious for COVID-19. Some vaccines worsen the consequences of infection rather than protect, a phenomenon called antibody-dependent enhancement (ADE). ADE has been observed in previous attempts to develop coronavirus vaccines. To add to the concern, antibodies typical of ADE are present in the blood of some COVID-19 patients. Such concerns are real. As recently as 2016, Dengavxia, intended to protect children from the dengue virus, increased hospitalizations for children who received the vaccine.”
Interestingly, they found that children with a certain “medium” level of antibodies to dengue fever were the ones experiencing ADE upon second infection. I’m not familiar with how antibodies work, so I’m wondering if we may still see ADE with these vaccines over time once vaccine antibodies have the chance to decline in vaccinated people and those people are then exposed to the virus. Have there been studies on people that have been infected with covid-19 twice? I am under the impression that it hasn’t happened too often yet, but maybe it will over time as antibodies do wane and/or variants circulate. Dengue virus is not a coronavirus, but it seems we still don’t know a lot about how coronaviruses work? We have a vaccine for the flu, but we weren’t successful in making one for SARS and MERS, right? Was there ADE occurring with those vaccine attempts? I’m trying to understand!
Also, what are toxic stabilized nucleotides, toxic pegylated molecules, etc.? Would these be likely to cause acute problems or chronic problems like autoimmunity? How long will it take for them to measure autoimmunity induction or will they?
Best,
Nikki
https://www.scientificamerican.com/article/scientists-solve-a-dengue-mystery-why-second-infection-is-worse-than-first/
https://science.sciencemag.org/content/358/6365/929
https://www.scientificamerican.com/article/the-risks-of-rushing-a-covid-19-vaccine/
Dear Nikki,
These older articles were from before the 2020 US election. They were never motivated by science, but by politics: Democrats were worried that Trump would pressure the FDA to approve the vaccine before the election and thereby appear a hero.
When these articles were published, it was *already* abundantly clear from epidemiological data that prior infection with COVID was highly protective against future infection. Contrast this to the situation with dengue fever, where prior infection tends to make future infection worse. If prior infection makes future infection worse for dengue fever, is it any surprise that vaccination against dengue fever can make future infection worse? But if you already know that prior infection is greatly protective against future infection for COVID, then why do you think dengue fever vaccines are a good model for COVID vaccines? Especially because, as I mentioned above, the situation with dengue fever is the exception rather than the rule, and tends to occur for viruses with tropism for immune cells like dengue fever and not like COVID.
Anyway, back when these articles were published, they were pretty clearly in the realm of politically-motivated speculation, not in the realm of science. Now they have been directly contradicted by hard scientific data — both the clinical trial data, and epidemiological data from our vaccine rollout. In other words, these concerns were never relevant, and new research has only confirmed their irrelevance.
By the way, the reason we weren’t successful in making a vaccine for SARS or MERS is that the threat disappeared, and funding dried up, before we succeeded. The research on SARS and MERS did was essential in making the COVID vaccines, and was the reason we succeeded so quickly.
Best,
-Eric
That’s interesting, Eric! Thanks for the response. I am like Yulia and feel I won’t be able to wait and watch forever. You sound like you are very convinced of the research, but I do wonder why Paul still has reservations if it is truly a closed case. Just curious! I learn a lot from reading everyone’s questions and input. Best, Nikki
Hello Paul,
Thank you for your response. How could the stabilized nucleotides become toxic? Would the “expression of toxic viral proteins” and the inflammatory attacks on cells that express the spike protein also be issues for infection with the actual virus, as well, or just the spike protein from the vaccine?
Now that we are in beginning of June, any updates on your thoughts on the results we are being presented with in terms of decreased death/hospitalizations in the vaccinated lending to these vaccines being safe? Perhaps looking at the data coming from Isreal, for example?
Do you have an opinion on what Eric Larson wrote?
Thank you for your input, as well Eric Larson.
Kind regards,
Yulia
Thanks for taking the time to provide this info, Eric.
I was on the fence for the longest time weighing the risks/benefits of both sides.
Finally received first dose of mRNA vaccine a few days ago. The negative psychological effects I was experiencing from going back and forth undecided were way worse than the actual shot.
Had my epi pen with me but thankfully wasn’t needed. Slightly sore arm for a couple days but otherwise no flare ups of any previously healed health conditions so far (had severe mast cell activation years ago that I was stuck with for several years but is now in remission).
Following the emergence and spread of the Delta variant really pushed me off the fence. I do not want my body’s first encounter with COVID to be the Delta variant or the next more serious variant without giving it some instructions first. I felt there was just no choice but to get the vaccine. I am willing to accept any potential negative effects of the vaccine because I feel natural COVID infection is so much more damaging and I would like to avoid death or becoming chronically ill again.
https://twitter.com/Bob_Wachter/status/1404151502864883713
For those still on the fence please stay safe and don’t let down your guard this fall/winter.
Hi Eric, if you see this was wondering if you saw Paul’s latest comment on the vaccine in the PHD facebook group? It is quite dark and alarming.
I’m still confident in the decision I made for my personal circumstance. The Delta variant is an immediate threat to the unvaccinated and those without immunity from previous COVID infection.
Hi Paul,
I’m genuinely curious if you’ll be:
1) Pursuing natural immunity via COVID infection (potentially dangerous outcome as the severity of variants increases with probable long term negative health effects and not as durable immunity)
2) Waiting for a different vaccine. What do you think of Novavax? Is there another one in the pipeline you’re interested in?
3) Avoiding COVID infection indefinitely (increasingly difficult as variants become more transmissible and countries transition to opening)
I considered the third option but don’t wish to remain isolated indefinitely. Continuing with properly sealed N95 masks/eye protection to protect against airborne transmission whenever out in the world is possible but situations can arise that aren’t 100% in one’s control. Vaccine immunity is a great safety net.
Unfortunately, for the average person COVID is a very real threat and vaccination is their best chance at living life today. Most don’t have the luxury of basing their decision on a hypothetical future doomsday scenario. Vaccines, including the mRNA ones, will be used by people all over the world. So the scenario you mentioned in the facebook group would equate to mass global extermination. Isn’t China even looking into developing their own mRNA vaccines since those ones are still performing stellar against the variants to date (with two doses) and can be pivoted to address new variants if needed? This is truly a global fight for the future of humanity. (Hi from Canada where we’re absolutely rocking it on the vaccination front)
This is a worthwhile article that discusses what lies ahead:
https://www.foreignaffairs.com/articles/united-states/2021-06-08/coronavirus-strategy-forever-virus
Unfortunately, globally it’s going to be difficult to get rid of this virus for good. So I think I’m going to have to get used to the idea of taking vaccines whenever they’re necessary for personal protection and to contribute to the health of the community. We are incredibly privileged to now have effective vaccines that are safer than natural COVID infection available to us.
Anyway, respectfully interested in how you plan to navigate this going forward. Take care.
I haven’t been following these wellness communities closely lately but I found this a really great in depth overview of the mRNA vaccines backed by current evidence. Especially for those like myself who are worried about potential flare ups of past or current medical conditions:
https://www.thepaleomom.com/the-covid-19-mrna-vaccines/
@Eric Larson & Paul
Thanks for the pro & cons of vaccines. What’s your take that mRNA vaccines are supposed to damage the blood vessels? https://www.youtube.com/watch?v=5sIWb9GTbbE&t=1s
Hi MArk,
Clinically significant damage of the vasculature to the extent that Hoffe claims would be apparent from both the clinical trial and epidemiological data, both of which are large and robust data sets. But it simply isn’t there.
Without a more detailed presentation of his data, I’m not sure where Hoffe went wrong. But I can speculate: It sounds like there is no good control group for his study. The number of participants might be unrepresentative of the general population in important ways, or extremely small (you could get 62% from 5 participants out of 8). His proposed mechanisms, and his claim of clinical significance for an elevated D-dimer test, are quite speculative. And the basic biology errors that he makes, e.g. claiming that capillaries cannot be regrown, do not inspire confidence. (Here is the wikipedia article on capillary regrowth: https://en.wikipedia.org/wiki/Angiogenesis)
As I said before, the clinical trial and epidemiological data show quite clearly that direct adverse effects of the vaccines are minimal. What Hoffe says is far less convincing.
Best,
-Eric
Thank you for all your comments, Eric. Many people have legitimate concerns that you’re helping to address with detailed explanations. I was extremely vaccine hesitant and got my second dose yesterday. I’ve resorted to watching medical creators on TikTok to cope with the rampant misinformation. I’m disappointed with many influencers in the ancestral and integrative health communities.
https://www.tiktok.com/@laughterinlight
https://www.tiktok.com/@dr.eric.b
https://www.tiktok.com/@christinaaaaaaanp
https://www.tiktok.com/@dr.noc
https://www.tiktok.com/@scitimewithtracy
https://www.tiktok.com/@drsiyabmd
https://www.tiktok.com/@dr.jon.l
https://www.tiktok.com/@beachgem10
https://www.tiktok.com/@epidemiologistkat
https://www.tiktok.com/@dr_asherwilliams
https://www.tiktok.com/@musclesandnursing
https://www.tiktok.com/@jesss2019
https://www.tiktok.com/@thatsassynp
Take care everyone!
Highly recommend ‘This Week in Virology’ podcast for scientific and clinical COVID-19 updates.
https://www.microbe.tv/twiv/
Came across a short video on Charles Hoffe if anyone is interested. It doesn’t look like his data is published for scientists to review.
https://www.tiktok.com/@dr.jon.l/video/7011331920722267398
Dear Paul,
I think you were right back in April. Your statement below alarmed me. It contradicted what I heard from the media and major institutions, but so is your diet advice. 🙂
“There are a variety of pathways by which the vaccines could cause problems, including toxic stabilized nucleotides, toxic pegylated molecules, expression of toxic viral proteins, induction of inflammatory attacks upon cells expressing the foreign protein (which is needed for the vaccines to generate immunity), induction of autoimmunity, and of course antibody-dependent enhancement of infections.”
Stay well,
Rose
Thanks, Rose. You’re not the only one who doubted, several of my immediate family members got the vaccines and one spent several weeks in ICU and required three cardioversions.
I think when people realize that the Regeneron neutralizing antibody cocktail, which delivers every potential benefit of vaccination at zero risk of side effects, could have been delivered to everyone at hardly greater cost than the vaccines; that the vaccines have potential for severe adverse effects which may in some cases be life long; and that the efficacy of vaccination may soon go to zero or even become negative as viruses that are unaffected by or even amplified by a vaccinated immune background begin to circulate — in other words, when people realize they’ve been harmed by the vaccines to no productive purpose — there is going to be considerable and justified anger. It will be even worse if people discover that alternative constituents may in some cases have been substituted for the vaccine mRNA in order to conduct large-scale clinical experiments on an unsuspecting and uninformed population (how, for example, were the recently seized 1.6 million Moderna vials in Japan containing stainless steel nanoparticles “contaminated” with these compounds?).
Best, Paul
I thought monoclonal antibodies, although great, aren’t as effective or as cheap or as safe. Don’t they have to be administered as early as possible or there can be worse outcomes? It’s my understanding that they’re currently used as a treatment not prevention meaning you have to get infected first. I’m aware of a long-acting antibody combination pre-exposure prophylaxis for immunocompromised and vulnerable populations.
https://www.astrazeneca.com/content/astraz/media-centre/press-releases/2021/azd7442-request-for-emergency-use-authorization-for-covid-19-prophylaxis-filed-in-us.html
https://www.astrazeneca.com/content/astraz/media-centre/press-releases/2021/azd7442-phiii-trial-positive-in-covid-outpatients.html
Hopefully they can eventually make it pan-sarbecovirus antibodies so that it doesn’t select for resistance. This looks more promising to me especially when people with infection-induced immunity start getting reinfections.
https://twitter.com/jefftownsend/status/1445082321410039823?s=21
These therapies aren’t widely available in Canada yet and don’t seem feasible to mass distribute globally? In contrast scientists are working on oral and intranasal vaccines that could be delivered to developing countries.
https://twitter.com/stephanielangel/status/1445503905358512128?s=21
Could you explain your concerns in a little more detail with studies to help me understand? Thanks!
(Just throwing out thoughts please correct me if I said anything stupid, Eric.)
Hi Alexandria,
Neutralizing antibodies are highly effective, non-neutralizing antibodies are inflammatory and against coronaviruses can be harmful as well as beneficial. The vaccines are less consistently effective than neutralizing antibodies, as not everyone produces neutralizing antibodies in response to vaccination, and have a considerably worse safety profile.
Antibodies are easier to produce consistently than the lipid nanoparticle mRNA vaccines, if they aren’t widely available it’s because governments haven’t wanted them to be.
Best, Paul
Just wanted to make a correction to my previous comment that just today monoclonal antibodies became available in Canada if you meet specific criteria.
https://twitter.com/kashprime/status/1452606513621749761?s=21
This is awesome but I don’t understand how this is a either-or thing with vaccines when both can be used. 49.9% of the entire world population have now received a vaccine (more than 3.83 billion people) but still a very low % in low-income countries.
Hi Paul.
Do you have any thoughts on how dangerous Covid actually is? You may have heard that John Ioannidis at Stanford estimated an infection fatality rate of 0.15% which is obviously very low but was much criticised by colleagues for that paper. But, as you probably know, he has throughout his career been hugely respected and it’s difficult to fully trust the medical establishment who rounded on him. Meanwhile, Joe Rogan, in a recent podcast with the much maligned (but truly independent) journalist Alex Berenson, noted that 95% of Covid deaths in the US were in those with at least FOUR co-morbidities. Not sure of his source for that.
I’d also like to ask – as well as the dangers of ADE, I’m guessing you’re also aware of the Marek effect observed in certain viruses in chickens, which makes the disease far worse for unvaccinated chickens while vaccinated chickens are protected. This is obviously the opposite problem to ADE – do you think this is also a possibility with Covid vaccines? Dr Geert vanden Bossche has discussed the folly of mass vaccination during a pandemic and believes it presents dangers for both the vaccinated and unvaccinated https://www.geertvandenbossche.org/
With each passing month, I become more and more convinced that I made the right decision in refusing the vaccine, after listening to you, Chris Masterjohn and Anthony Colpo (who admittedly appears less measured than you and Chris but provides valuable insight nontheless!) However, I did have my wobbles at times this year – I’m not aware of anyone whatsoever among friends and family who isn’t double vaccinated. I’m alone!
The censorship, and the complicity of the media in stifling open discussion of many aspects of the pandemic, has been shocking and makes me feel pretty uneasy. For 32 of my 34 years on this planet, I thought we in the West had a free and unbiased media. I just wish we knew WHY this was happening. Hopefully it’s just incompetence and good old-fashioned Big Pharma lobbying (corruption). But it’s becoming harder not to believe something else might be afoot, whether orchestrated by China / globalist interests linked to WEF/ both. This post ended up becoming more political than intended!
Hi Harry,
Biology is complex and many things can happen. I would suggest that you won’t go too far wrong by watching the Chinese and copying what they do. They know the most about this virus and its interaction with vaccines. To date, China has not allowed any mRNA vaccines to be administered.
Best, Paul
Thanks Paul.
Obviously, one curious thing about China is that it’s the only country in the world (looking at data on Worldometer.com) which has avoided a second wave, let alone a third wave, of the virus. This could be:
1) because their data is fabricated (and they have suppressed reporting of further waves);
2) because their strict non-pharma interventions e.g. draconian lockdowns, are effective;
3) because they haven’t used MRNA/AAV vaccines;
4) because, as one scientist whose work I subscribe to on Substack has interestingly speculated, they may have rolled out airborne treatments to their population which we don’t know about. Fascinating, if a bit sci-fi.
Obviously, this might not be an exhaustive list. I think uncovering the reason for their success would be most instructive.
Hi Paul and Harry,
1. I’m not sure where you got your information on the price of vaccines vs antibody cocktails, but it is orders of magnitude off. The US government purchased the vaccines in bulk from Moderna/Pfizer for about $20/dose, and the antibody cocktails in bulk from Regeneron for about $1250/dose. The vaccines are *vastly* cheaper than the antibody cocktails.
2. The efficacy of the mRNA vaccines is also *higher* than the antibody cocktails. In clinical trials against earlier strains, about 95% for the vaccines vs about 80% for the antibody cocktails if administered preventatively. With delta, the efficacy of both has fallen (the vaccines to about 88% and not sure off the top of my head how far the efficacy has dropped for the antibody cocktails). This is because antibodies are only one component of the immune response. In other words, the vaccines may induce a less-optimized antibody profile, but they also induce cellular immunity which more than makes up for the difference.
3. I’m not sure why China has done so well, but my bet would be on (2).
Best,
-Eric
Hi Eric, I’ve updated my comment. #2 needs a fuller response than I can give at present. “Efficacy” is a vague term by itself (what endpoint?) and by the standards that patients care about, their health, I think the antibody cocktails are a much better deal.
Best, Paul
Thanks Eric.
Do you have any concerns about the possibility of vaccinated people becoming dependent on regular booster vaccines for immunity to Covid? Or do you share none of these concerns about vaccine safety/efficacy? Another concern that has been shared recently in vaccine-skeptic circles is the exceptionally high number of excess deaths in younger age groups in European countries at the moment, which can’t be accounted for by Covid deaths: https://www.euromomo.eu/graphs-and-maps
On China’s pandemic management, why do you think no other country, across all political and social cultures, has managed to prevent similar outbreaks with non-pharmaceutical interventions?
Hi again Eric
For clarification, do you believe someone vaccinated 6 months ago has 88% reduced risk compared to an unvaccinated person, or that someone who is experiencing peak immune protection (say two weeks after second jab) is experiencing the 88% risk reduction?
If the latter, what do you think is the risk reduction for those, like both my 95-year old and 101-year old Aunts, who received their 2nd doses in April, six months ago? Do you think it’s likely 0 already (assuming they haven’t had their booster jabs)?
Thanks!
Hi Harry, If you listen to Chris consider also following AviBittMD on Twitter. He’s been correcting Chris for months and keeps challenging him to debate. Like Eric, he’s very open to answering questions and explaining in detail.
https://twitter.com/AviBittMD/status/1448831535323484168
Thanks Alexandra. I’m following him now.
Hi Harry,
1. I’m not concerned about the need for regular boosters. We get regular boosters for influenza already. Why would regular boosters for COVID-19 be so bad?
2. What other countries have as much state capacity as China? In the US, like in most of the west, the government can barely rename a post office.
3. The 88% figure is my best guess at *average* efficacy against *symptomatic* disease over the first 6 months. So if you are looking at the subset of people at the peak of their immunity, it would be higher than 88%; if you are looking at the subset of people 6 months later, it would be lower than 88%. If you are looking at efficacy against severe disease, it would be higher (wane more slowly); if you are looking at efficacy against asymptomatic disease (as judged by positive PCR test), it would be lower (and wane more quickly). If you are looking at elderly individuals, it would be lower and wane faster; for younger individuals, it would be higher and wane more slowly.
So no, the risk reduction for your aunts is definitely not zero already. Probably something like 70% vs symptomatic disease, and 90% vs severe disease? But that’s an off-the-cuff guess, not looking at any actual data right now. I’d still get the booster though, which would increase that even further.
Best,
-Eric
Hi Paul
If these vaccines carried a risk of illness as high as, or higher than, that caused by the virus itself, wouldn’t the statistics be showing noticeable levels of hospitalisations of vaccinated people by now, especially in countries such as Israel which have vaccinated a significant proportion of their population? Or might this take longer to show up in the stats?
Hi Harry,
I think we should have an idea within the next few months of how dangerous the vaccine-specific post-injection effects are.
Then, it will take some time to compare death rates from COVID among vaccinated vs unvaccinated.
I think by the end of the winter we should know or have a good idea.
Best, Paul
Hi Paul
It’s early days still but this article on UK vaccination data suggests the vaccines might indeed be safer than taking your chances with the virus:
https://www.bbc.co.uk/news/health-56153617
The researchers have come up with a figure of 75% reduction in risk of hospitalisation and death. (We’re currently using the Pfizer and AstraZeneca vaccines here in the UK and more than 25% of the population has had the first dose of a vaccine).
I really don’t know how to square this with Anthony Colpo’s enlightening articles about the poor testing of these vaccines (and of the US CDC’s and Public Health England’s conflicts of interest…)
Hi Paul,
I wanted to circle back on this comment since it’s been some time and vaccine rollouts are moving along swiftly with a large number of people already vaccinated.
Do you still feel the mRNA vaccines are not safe?
Hi Paul
Do you think it’s plausible that those in whom the rest of the immune response (besides the antibody-mediated) is robust and healthy would be less likely to suffer the effects of ADE (antibody-dependent enhancement)? I assume, if so, PHD would as usual be the best prescription for this, with an emphasis on adequate vitamin D levels for the cell-mediated response?
I plan to gently warn my family, who have been vaccinated, about this possibility and would like to sweeten the news with advice on how to minimise the risks!
Despite my comment here in February, with a link to the BBC article suggesting these vaccines are very effective, I’ve decided it seems the benefits probably don’t actually outweigh the risks for a healthy-weight 33 yr old who follows your very immunity-optimising diet – even if the vaccines are exceedingly effective at minimising Covid risk and ADE doesn’t become a complication of them. In fact, I’d actually like to request that you delete that earlier post but understand if you prefer not to delete comments.
We are living in truly worrying times so thanks for continuing to share your wisdom on this. I’d imagine your cancer treatment drug is being tested more thoroughly! 😄
Hi Harry,
I shortened your name on the previous comment so that it will be more anonymous, I think it was a reasonable comment and would prefer to leave it but can delete it if you wish.
I do think PHD is a good defense against COVID. I doubt whether anyone who had been on PHD for a while would be likely to die from the COVID variants we have seen so far. In general, nourishing natural whole foods diets that are low in omega-6 fats will tend to generate an optimal immune response.
The problem with antibody dependent enhancement, ADE, is that it is a feature of the virus not the immune response. A virus that can prevent killing by phagocytic cells, but rather reproduces effectively in phagocytic cells, will be amplified by vaccination antibodies rather than suppressed. If COVID was an engineered virus, China may have many variants of the virus that they tested during its development, some with ADE and some without. An agent with ADE capability could then be released at a later date, in which case vaccination would backfire.
There may already be variants with ADE circulating, see e.g. https://www.lifesitenews.com/news/death-rate-from-variant-covid-virus-six-times-higher-for-vaccinated-than-unvaccinated-uk-health-data-show. It’s notable I think that less than 3% of Chinese have been vaccinated. The Chinese government may know that vaccination is undesirable.
The bottom line, I think, is that we need good therapies against infectious agents including COVID.
Yes, indeed, our cancer therapy has been tested far more thoroughly than these vaccines, and we’re very excited about it.
Best, Paul
Thank you Paul!
Hi Paul,
It looks like vaccination *lowers* the fatality rate from the Delta variant by about 70%. So this is evidence *against* ADE with the Delta variant.
Source: Tables 10 and 11 from the document that the lifesitenews article disingenuously claims to be reporting on, but at least helpfully links to. Keep in mind that vaccine supplies were allocated initially to the most vulnerable (the elderly and those with underlying medical conditions). So comparing raw fatality rates is completely inappropriate here, and you need to use appropriately-matched controls.
As an illustration of what is going on here, look at the raw data for hospitalization rates with just two buckets:
—
(Age under 50 & unvaccinated): 0.7%
(Age under 50 & fully vaccinated): 0.4%
(Age over 50 & unvaccinated): 5.6%
(Age over 50 & fully vaccinated): 1.8%
—
(Any age and unvaccintated): 0.8%
(Any age and fully vaccinated): 1.0%
—
It’s a nice illustration of https://en.wikipedia.org/wiki/Simpson%27s_paradox
Best,
-Eric
Thanks Eric! That’s what I get for stopping at the headline.
The basic point though remains, there is potential for a coronavirus variant to emerge (or be introduced as an agent of biological warfare) that hits the vaccinated harder than the unvaccinated. It’s a reason to be cautious about vaccination apart from considerations of immediate safety or efficacy against the extant strain of coronavirus.
Update – just noting that according to this doctor, Public Health England data shows the death rate the Delta variant is 2x higher among the vaccinated than among the unvaccinated. https://twitter.com/arkmedic/status/1406075170595295232.
We’ll eventually learn whether the Delta variant exploits vaccination, but what is concerning is the potential for eventual emergence or release of variants with death rates far higher among the vaccinated – 10x or more. We need good therapies before that happens.
Paul,
I am very surprised to hear you think that less than 3 percent of Chinese have been vaccinated. According to the New York Times, China is trying to vaccinate 40 percent of its citizens by the end of this month.
That is a very large number considering its population.
I appreciate information coming from you and would love to hear more….
Thank you,
Rose
Hi Rose,
I may be out of date, I was recalling that percentage from this article which dates from March: https://qz.com/1981186/chinas-covid-19-success-is-slowing-its-vaccine-rollout/.
Apart from the number vaccinated, it’s also notable that China has not allowed any of the Western vaccines to be used in China, and has approved four Chinese vaccines, all notably ineffective. It is likely that China desires its vaccines to be ineffective. They are not inferior to the West in their capabilities.
Best, Paul
Really appreciate the discussion.
Here’s an article from The Associated Press:
https://apnews.com/article/china-gao-fu-vaccines-offer-low-protection-coronavirus-675bcb6b5710c7329823148ffbff6ef9
Gao Fu, China’s top disease control official, made some comments of interest a couple months ago. Here are some quotes from the article:
“We will solve the issue that current vaccines don’t have very high protection rates,” Gao said in a presentation on Chinese COVID-19 vaccines and immunization strategies at a conference in the southwestern city of Chengdu. “It’s now under consideration whether we should use different vaccines from different technical lines for the immunization process.”
He also praised the benefits of mRNA vaccines, the technology behind the two vaccines seen as the most effective, Pfizer-BioNTech and Moderna, months after questioning whether the then-unproven method was safe.
Health officials at a news conference Sunday didn’t respond directly to questions about Gao’s comment or about possible changes in official plans. But another CDC official said Chinese developers are working on mRNA-based vaccines.
“The mRNA vaccines developed in our country have also entered the clinical trial stage,” said the official, Wang Huaqing.
Gao concluded his presentation Saturday with praise for mRNA vaccines and called for innovation in research.
“Everyone should consider the benefits mRNA vaccines can bring for humanity,” Gao said. “We must follow it carefully and not ignore it just because we already have several types of vaccines already.”
It’ll be awesome when more mRNA vaccines are approved and also demonstrated to be safe and effective. Then outbreaks of specific variants can be more quickly targeted across the globe with greater production capacity. 😀
This article from a few days ago speaks to the status of China’s approvals of foreign vaccines:
https://www.scmp.com/news/china/science/article/3137662/will-slow-approval-biontech-and-other-foreign-vaccines-block
Can be read fully through archive:
https://archive.is/eXiJh
Hi Paul,
Wouldn’t the inactivated virus vaccines used in China carry the same risk of ADE from a future strain?
This study in cell was recently published and seems encouraging: https://www.cell.com/cell/fulltext/S0092-8674(21)00756-X
Hi Paul,
The twitter thread you linked to is discussing the same dataset — and makes the same mistake — as the lifesitenews article you linked to earlier. In fact, the PHE data shows vaccination is strongly *protective* against Delta (as it is against every other circulating strain): The estimates are about 80% protective against disease, on top of about 70% reduction in fatality rates, for a total mortality reduction of about 94%.
As I explained before, it is completely inappropriate to compare raw fatality rates, given that the vaccine was allocated on basis of vulnerability. If you want a precise estimate of vaccine effectiveness, you need to use properly matched controls. If you just want to convince yourself that Delta is not exploiting vaccination, then it suffices to separately consider those under/over age 50 (as age is the single greatest risk factor for mortality).
Best,
-Eric
—
Hi Nikki,
No. Most cases of vaccine-induced ADE are seen with inactivated virus vaccines, like those used in China.
The reason is that inactivated virus vaccines do not induce a robust T-cell response. This means they are simultaneously *less* effective, while posing a *greater* risk of ADE against future strains. It’s a lose-lose situation.
Surely the Chinese scientists know this — but no amount of scientific knowledge could help here, because that is not what is lacking. An approval of foreign vaccines would be a sign of weakness.
—
Best,
-Eric
https://www.nytimes.com/2021/06/25/opinion/coronavirus-lab.html
https://archive.is/O5Xej
“The secrecy and the cover-ups have led to some frantic theories — for example, that the virus leaked from a bioweapons lab, which makes little sense, since, for one thing, bioweapons usually involve more lethal pathogens with a known cure or vaccine, to protect those who employ them.”
“But a better path forward is one of true global cooperation based on mutual benefit and reciprocity. Despite the current dissembling, we should assume that the Chinese government also doesn’t want to go through this again — especially given that SARS, too, started there.”
https://www.bloomberg.com/news/features/2021-06-27/did-covid-come-from-a-lab-scientist-at-wuhan-institute-speaks-out
No opinion on this whole accidental lab leak vs. natural origin debate but the bioweapon scenario just doesn’t make any sense to me since as Eric pointed out future variants could hit China’s vaccinated population (and the numerous countries they are sending vaccines to) harder without appropriate boosters. Really wish SARS-CoV-2 would stop being an absolute jerk at every opportunity.
Hi Alexandra,
My guess would be an accidental lab leak. The initial cases of COVID-19 were distributed along the #2 subway line in Wuhan, which services the Wuhan Institute of Virology. Several researchers at the Wuhan Institute of Virology were hospitalized with pneumonia in November 2019, right before the pandemic officially began. If COVID-19 were of natural origin — or was released intentionally — then both of these would be fairly unlikely coincidences. I assume that researchers will be more careful going forwards, or that the government will force them to be, now that they have seen the consequences. So a further accidental leak seems thankfully unlikely. Our main worry with COVID going forwards is natural evolution of variants, which will likely arise because not enough people have been vaccinated yet to reach herd immunity.
Best,
-Eric
Hi Paul, Eric, and the rest. Thank you for engaging in discussion. I find it difficult to find information that doesn’t fall either into senseless quackery or into blind faith in authority. This has been educative.
From a recent Anthony Colpo post;
“I’ll let the Delta infection and death figures, also from the UK Technical Briefing referred to above, speak for themselves. The table containing the Delta infection rates in vaxxxinated vs non-poisoned individuals can be found on page 13 and 14 of the document.
The table shows that at 28 days, 53,822 of the 92,029 documented Delta cases were in unvaccinated people. So at first glance, it appears the unvaccinated are at higher risk. But a closer look at the figures tells a very different story.
The higher case numbers applied to under 50s only; in the over-50s, more people with Delta infections had received the clot shot (3,954 vaxxxinated versus 3,546 non-injected).
The over-50 data is cause for concern in itself, but to get a true grasp of how useless and counterproductive the vaxxxines are, take a good look at the death figures below, taken from page 14 of the report. Despite a far lower overall number of people with Delta infection, the vaccinated groups have a far higher overall rate of fatality.
Of 117 deaths, 20 were in those who received one dose of the clot shot, and 50 of those occurred in those who were double-jabbed.
In total, 70 of those who received one or two vaxxxine jabs were subsequently rewarded with a left hook from hell.
In contrast, only 44 of the Delta deaths occurred in unvaccinated folks. But 68% of Delta infections were recorded among the unvaxxxinated, which indicates a powerful death-potentiating effect of the vaxxxines.”
https://anthonycolpo.com/conjob-21-why-everything-youre-being-told-about-the-delta-variant-is-complete-nonsense/
Hi Darrin,
Anthony’s “analysis” is based on the same data set as we have been discussing the entire time above. In fact, this data set shows the vaccines are strongly protective against the Delta variant. I suggest you reread my comments above.
But Anthony’s “analysis” is a new low in statistical illiteracy. He doesn’t merely make same the mistakes as the lifesitenews article and the twitter thread discussed above. In addition to those mistakes… He actually compares the death *counts* between the vaccinated and the unvaccinated! Not the death *rates*! For example, if we compare the number of COVID deaths among people whose name starts with ‘A’ to the number of COVID deaths among those whose name doesn’t start with ‘A’, which do you think will be greater? (Hint: Which group has more people? If the same fraction of each group dies, which group will have more deaths?) Does that mean having a name that starts with ‘A’ is protective against COVID? By Anthony’s method of “analysis”, yes! This is why it is essential to compare death *rates*, not death *counts*.
Best,
-Eric
… so we cannot make any conclusions from the 109 c-19 related deaths in the over 50’s… not enough data(?).
Hi Darrin,
No, the 109 deaths show the vaccine is *protective* against Delta. Of the 109 Delta deaths in those over age 50, we have:
– 50 deaths in fully vaccinated individuals
– 18 deaths in partially vaccinated individuals
– 38 deaths in unvaccinated individuals.
(The remaining 3 deaths occurred in patients whose vaccination status was unknown.)
On the other hand, of the population over the age of 50 in England, roughly 85% is fully vaccinated, roughly 5% is partially vaccinated, and roughly 10% is unvaccinated. So the *rates* are proportional to:
50/85 = 0.59
18/5 = 3.6
38/10 = 3.8
So someone over age 50 who is fully vaccinated is 3.8/0.59 = 6.4 times *less* likely to die of the Delta variant than someone who is unvaccinated, in this data set.
And that’s going to be an underestimate of true vaccine efficacy against mortality, because the vaccine was allocated on basis of age and vulnerability. Indeed, even once you restrict to those over age 50, full vaccination rates range from under 80% in those age 50–55 to over 90% in those 70 and older. To put it another way, vaccinated individuals over 50 are 6.4x less likely to die of Delta… even though they are on average older and were less healthy before they had the choice of vaccination.
Best,
-Eric
Hi Eric,
I’ve found your comments so helpful. There are a couple PHDers in the facebook group who have said they know of safe and effective treatments for COVID and that the vaccines are “poisons.”
I hope you don’t mind but I referred them over here to discuss their data with you. This is what I said:
“On the PHD website comments section, myself and many others have found Eric’s analysis of data really insightful and reasonable. If either of you has a way to prevent COVID infection and transmission besides vaccination + continued masking I would encourage you to discuss it with Eric. If he agrees with the data you present to him then many PHD readers over there might find that information helpful. We need as many effective therapies as possible to throw at this thing. I hope more medical advances continue to be made.”
Hope to continue the discussion over here so that we can all learn!
Hi Paul,
I just want to say thank you for providing a lively and nonjudgmental (rare) forum for us to discuss health in general and now COVID in particular.
There’s too much noise out there from either end of the COVID vaccines’ spectrum. It’s literally giving me a headache. So, thank you for giving me a virtual space to go to for relief.
I’m also incredibly grateful to Paul for this forum and everyone’s respectful contributions despite differing opinions. It has been enlightening to have the emotion and noise removed and to attempt to look at the facts and data. Thanks all!
This seems like really promising research:
“Scientists have uncovered an antibody that can fight off not only a wide range of SARS-CoV-2 variants, but also closely related coronaviruses. The discovery could aid the quest to develop broad-ranging treatments and vaccines.”
https://www.nature.com/articles/d41586-021-01917-9
I wonder if this changes Paul’s opinion? China was extremely diligent and cautious reviewing the safety of this vaccine and it is kind of embarrassing for them to approve a foreign mRNA vaccine due to vaccine nationalism so they must think it is really necessary.
Coronavirus: BioNTech may become first foreign vaccine approved for use in mainland China
-The panel advising the country’s regulator gave the green light to the jab, which will be the first using cutting-edge mRNA technology on offer on the mainland
-China looks set to use the drug as a booster for those who have received two shots of home-made vaccines
https://www.scmp.com/news/china/science/article/3141228/biontech-track-become-first-foreign-covid-19-vaccine-approved
Article can be read fully here for more details:
https://archive.is/Wcara
Interesting advice:
https://www.facebook.com/lissarankin/posts/375290207292186
^ that FB post mentions herd immunity…
As far as I can tell,
sterilising vaccines are required for any chance of achieving herd immunity (if using vaccines).
& like flu vaccines, covid vaccines are Not sterilising vaccines.
… & like flu vaccines, the best we can hope for with covid vaccines, is reduced symptoms, & reduced hospital admittance.
I think you could be right, Darrin…
Do you think a universal, multi-variant coronavirus vaccine and/or nasal spray vaccine could get us closer to sterilizing vaccines?
This is part of some posts I made in the facebook group. If anyone has anything to correct or add please let me know since I’m not a scientist!
I’m glad we can both agree that COVID is real and masks are important right now. Yes, 39% at preventing infections from the Delta variant in Israel (it’s still higher in countries that vaccinated later). From that same dataset the vaccine still provides very high levels of protection against hospitalization (92%) and severe illness (91%). That’s why N95 masks are still needed for an additional layer of protection. New variants can emerge that evade vaccine-induced and natural immunity but for now the vaccines are still holding up well against a variant they were not designed for.
I’m looking forward to following the results of additional ivermectin trials like the one _____ just posted. I’m skeptical of it but really hope it helps. Ivermectin would NOT be appropriate for pregnant women to take at that dosing schedule for a significant length of time since it’s a category C by the FDA and known to cause birth defects in pregnant animals or people taking medications that interact with it. Like we discussed previously in this thread pregnant women and their babies are at increased risk of severe COVID outcomes and vaccination is advised.
https://drive.google.com/file/d/1_wHIYX-tGkGBPwuax7N8BxZPR4PTTCDm/view
https://elemental.medium.com/ivermectin-for-covid-19-an-update-5e913bb49483
This is likely going to become an endemic virus so updated vaccines and new treatments will be needed. Boosters have a really high likelihood of dramatically increasing protection. I respect your personal decision not to take the vaccine since you’re taking other precautions to prevent transmission and I hope in the future you can respect the decision of others to take the vaccines since they are saving lives and keeping people out of the hospital. Overwhelmed hospitals are affecting people who need treatments for other medical conditions and emergencies.
Among highly vaccinated populations the mutation frequency of the Delta variant is lower. A super variant that could threaten us all is more likely to emerge in populations with lower immunity. With SARS-CoV-2 there is significant variability in infection-induced natural immunity. Some people develop good immunity, some people not at all, for some it drops off quickly and for some it lasts longer. The vaccine provides more consistent higher levels of immunity because of the controlled dose that can be boosted and more protection against the Delta variant than natural immunity alone. Vaccination against COVID is critical to suppress emergent mutations. So it also benefits you if more people get vaccinated as it will keep your community safer. I was happy to be vaccinated with no horrible side effects personally.
https://www.medrxiv.org/content/10.1101/2021.08.08.21261768v2.full-text
Here’s more research showing fewer mutations in vaccinated people:
https://www.medrxiv.org/content/10.1101/2021.07.01.21259833v1.full.pdf
Moderna efficacy hasn’t declined. Still has greater than 90% against cases of COVID-19 and greater than 95% against severe cases of COVID-19 at 6 months. Looks like Pfizer will need booster doses sooner and Israel has commenced boosters to restore high levels of immunity. Moderna and Pfizer mRNA vaccines are basically the same except Moderna has 3X the dose. Taking a booster of vaccine once a year is a lot easier than taking ivermectin twice a week indefinitely. Do we even know the long term impact of ivermectin at that dosing schedule on our gut microbiome because that’s important to most health-minded people.
Nothing to add except I wish I got the Moderna vaccine and lived in Iceland or New Zealand right now lol. I was really nervous to get vaccinated so I guess testing the waters with Pfizer’s smaller dose was better for me. I think a larger dose might be helpful for older individuals. Hopefully Eric can fact check for us.
I’m also really curious what the deal is with ivermectin. I see a lot of people claiming it’s a miracle cure for COVID being suppressed by the mainstream and that it could end this pandemic.
Hi Alexandra and A.A.,
Israeli policy was to require proof of vaccination for entry to indoor unmasked activities such as restaurants and bars. So in the Israeli data, unvaccinated individuals had significantly lower exposure to COVID-19 than vaccinated individuals. The studies finding low efficacy of the Pfizer vaccine are all studies from Israel that make no attempt to control for this.
For this reason, I would place more trust in the data from Public Health England (PHE), which estimates the efficacy of the Pfizer vaccine against symptomatic infection with Delta at 88%, with a 95% confidence interval of 78–93%. See: https://www.medrxiv.org/content/10.1101/2021.05.22.21257658v1.full-text
Moderna has claimed no significant decrease in efficacy against Delta. It is difficult for me to comment on this, because they have not yet published their data, or specified how much uncertainty there is in their estimate. Note that their original clinical trial had an estimate of 94% efficacy, with a 95% confidence interval of 89–97%. So it is entirely possible that any difference between Moderna’s estimate for the efficacy of their vaccine, and PHE’s estimate for the efficacy of Pfizer’s vaccine, is purely measurement error.
Sure, it is a priori plausible that, due to the higher dose, protection from Moderna’s vaccine lasts longer or fares better against the Delta variant than Pfizer’s. But a priori it is also plausible that, after a several months of no difference in efficacy between the two vaccines against the ancestral strain or the Alpha variant… there is still no difference in efficacy against the Delta variant after 6 months.
—
Wearing an N95 mask, or similar, when indoors around other people is great advice. (I do it myself.) COVID might evolve to get around vaccines… but it can’t evolve to get through an N95 mask, and N95 masks protect you against all other respiratory infections too.
Of course, most people won’t wear a mask indefinitely, so we should just… update building codes to require HVAC systems that can filter/ventilate indoor air at, say, a dozen air changes per hour, in every building. That would reduce transmission enough to eradicate the common cold, eradicate influenza, *and* eradicate COVID.
—
As was the case with hydroxychloroquine last year, much of the data suggesting a benefit of ivermectin was probably fabricated. See: http://steamtraen.blogspot.com/2021/07/Some-problems-with-the-data-from-a-Covid-study.html
We’ll have more data hopefully soon, but I’m not optimistic. Hydroxychloroquine didn’t work, Remdesivir didn’t work, and repurposing existing drugs as antivirals has proven a mostly-futile exercise in the past for other viruses. (As far as I know, despite many such drug repurposing attempts, Nitazoxanide against influenza is the only example that has ever been shown to actually work… albeit with results that aren’t really that impressive.) In the mean time, I would not take ivermectin for COVID, either prophylactically or as a treatment.
Best,
-Eric
Hi Eric,
This is extremely helpful information. Can I have permission to post this in the facebook group to provide clarification to my post with credit to you?
Thank you so much for your insight on this.
Hi A.A.,
Yes, you may post my comment to facebook.
Best,
-Eric
I kept seeing This Week in Virology podcast recommended to keep up-to-date with SARS-CoV-2 scientific developments. This was my first time listening and the latest episode was really interesting. Some parts were challenging for a non-scientist but fascinating.
TWiV 796: The vary hungry spike with Paul and Theodora
https://www.youtube.com/watch?v=r-v9qfZCqKM
Some topics discussed:
27:00 – 29:00- resistance & mutations
37:00- resistance, mutations & fitness cost to virus
48:00- immune evasion variants
50:00- *important information for anyone with prior natural infection considering mRNA vaccination*
57:50- booster doses
1:01:50- vaccination goals, more debate on boosters
1:14:00- population immunity, boosters again, hospitalizations, world vaccination
1:23:00- vaccine requirements, natural immunity re-infections, future waves, masking, kids & schools
1:32:00 – 1:37:20- resistance vs. antibody maturation, antibody response variability in population
Anyone know of Dr. Rhonda Patrick? These MedCram videos have been excellent. The most recent was an in depth discussion with her and covered many of the topics you all have been discussing above.
https://www.youtube.com/watch?v=pp-nPZETLTo
“I would suggest that you won’t go too far wrong by watching the Chinese and copying what they do.”
I had a good laugh about that one. China has such a great track record on things. What a joke.
Hi! I am going to start this diet soon. I want to know how my current morning juice may fit in. Each morning I juice 1 brocolli stalk and florets, 1 zuchinni, 1 golden beet, 4 sheets of kale, a knob of ginger and turmeric, 4 carrots, and 1 cucumber. Each day it comes out to more or less 24oz. What requirements does this fulfill for the daily diet you recommend?
Also, are chia seeds ok?
Hi Eric,
Juicing is fine, though eating the vegetables would be even better. Eating that many vegetables is certainly not a requirement — you don’t need that much — but I doubt there is harm in it.
Best, Paul
Hi! Are all the brands of vitamins you recommend equal quality? I see there are some differences in price and want to make sure I’m not putting toxic manufactured vitamins in me.
Hi Paul,
I was more asking, can those ingredients in my juice count towards my daily vegetable requirements, even though I’m fore-going the fiber?
THANK YOU
Eric Blitzer
Yes, they count. You are not forgoing all the fiber, there is fiber in the juice.
Wow, so in theory, I don’t have to eat vegetables, I can ONLY juice them and keep my “meals” focused on fulfiling the remaining daily requirements, like starch, meat, etc.?
Hi Paul,
For the oil consumption, if I cook the oil, does that count? Does some of it evaporate/get left on the pain?
BEst,
Eric
I believe Paul recommends using saturated or monounsaturated oils for cooking (coconut fat, duck fat, olive oil, palm oil…) and using the leftover oil left in the pan, where some fat-soluble vitamins may have remained, to make sauces to accompany the food. In any case, oil should not be abused as a source of calories, because the PHD recommends whole foods, not refined sources.
Oil does not evaporate, it is burned. If you see smoke, it is a bad sign that the oil is being damaged. Although damage can also appear in the oil even if you do not see smoke, as it happens in sunflower oil (which apparently has a high smoke point, but at low temperature cooking it already creates harmful cancerous substances). That is why using saturated or monounsaturated oil helps, since polyunsaturated fats, besides being harmful per se when too much is taken, are very prone to go rancid and get damaged by heat and oxygen.
Another thing that I think Paul recommends is that, if you cook for example a chicken or industrial pork, do not eat the fat that it releases, because it is polyunsaturated and when it is directly exposed to heat it is more easily damaged than if it remained in the matrix of the food. But fat released from other meat such as duck, or ruminant meat, is fine because it is low in polyunsaturated fat.
Finally, if you cook something for many hours, such as a bone broth (which some people cook for a whole day), the fat that remains on top is best removed when the pot cools down. This is because when exposed to heat and in contact with oxygen, they will most likely be damaged.
Hope that helps. The book is a terrific source of good information, I recommend you get it!
Hi Paul! Thank you for everything you do. Do you have any insight into Erythromelalgia? It’s a neurovascular disorder that I have, after living in toxic mold. Fermented foods (even quercetin) elicit flares, while probiotics and yogurt do not. I’d love to heal with Perfect Diet foods like Bone Broth one day! Thank you so much.
Hi Paul! Do you have any recommendations for Becherev’s disease? I have a friend in the early 30s who suffers from this, with great pain in the knees and back, and it is getting worse. People are saying that starches should be avoided for this diagnose – do you believe that also includes “safe starches”?
Greetings
Martin
Hi Martin
There are many posts on anklyosing spondolitis on this site. Start here:
http://perfecthealthdiet.com/2014/01/curing-ankylosing-spondylitis/
Hi Paul, thanks for everything – your work is helping me manage my girlfriends CFS/ME!
Do you have any thoughts on https://www.truniagen.com/
It’s a Nicotinamide Riboside supplement that claims to increase NAD+ levels, thus improving energy creation and fighting aging – strong claims!
I know that you’re against Niacin, but they claim that this doesn’t have the negative affects that Niacin can.
Would love to hear your thoughts on this?
Thanks so much!
Ben
PS If you have any other guidance on CFS/ME, I’d love to hear it too!!
I read that storing potatoes in the fridge allows enzymes to convert the starches to sugars. If one prepared potatoes this way, would it affect PHD’s starch recommendation?
If you store potatoes in the fridge before cooking them, yes, it does affect PHD’s recommendations on proportions of nutrients, since now the potatoes have some sugar, and less starch. But I don’t know how much starch will be transformed, and at what rate it will happen.
Anyway, even if not a lot of starch is converted, it can be a problem, because sugar can react during cooking to create nocive substances. If you cook potatoes that have been stored in the fridge, you will see they turn black.
So, if you want to store the potatoes in the fridge for some reason, it’s better if cut them into pieces and blanch them. This way the enzyme will be deactivated. This is what is done in the industry with potatoes sold frozen, and with other vegetables as well.
Now, the other situation is: you store the potatoes correctly, then cook them, and then you store them in the fridge, it’s perfectly OK and healthy. The enzymes will be destroyed, so the starch won’t become sugar now. Instead, a part of the starch will change its structure in the cold, to become resistant starch, which is a kind of fiber very encouraged by PHD’s recommendations.
You won’t have to eat the potatoes cold, since you can reheat them gently and the resistant starch will stay there.
Hey folks, another potato question. In the book, white potatoes are the specific type that is advocated. Why is this type advocated in place of other varieties?
I don’t think white potatoes are singled out in the perfect health Diet. My sense is that the general category is underground starches. This includes all potatoes in the near neighbors such as yams and sweet potatoes of many varieties. The essence of the category is that the food digest digests largely to glucose. Rice is an obvious exception to the underground aspect but still qualifies as safe starch in that when cooked is largely toxin free primarily because the toxins are removed in milling. Sweet potatoes have more fructose than white potatoes and so are somewhat closer to the sweet plant category. In the book you will see that suggested combinations of safe starches are suggested in a table as an example to help you understand the balancing act. My sense is that diversity is good and that eating a variety of safe starches including white potatoes red potatoes yeah arms sweet potatoes is encouraged. As well as rice.
Hello Paul
i’m interested in your book and i’m going to purchase. you are not advocating a fad diet like so many others (no this, no that)but wholesome nutritious food which is refreshing for a change.
I took a heavy course of antibiotics last year and since then my health has been bad. for the first time ever i have eczema on my hands and neck and i suffer from rosacea and very sensitive skin after cleansing with lukewarm water and mild soap. i now have constipation which i never had before as well as other immunity issues (urinary infection a few months back, swollen eyelids)…can i please ask why do you say no oats? i have to eat oats every day otherwise i won’t go….please what would you recommend?
Sarah
While you are waiting to see if Paul responds (they are busy trying to cure cancer!), I will say what I can to help as much as possible:
1) use the search box at the top right of the website page and search on:
oat
This will give you a large list of links containing discussions about oats. Very useful really as you can read everything the community has said about anything specific over more than 10 years. Can be super informative and is directly accessible to you now.
The reason oats are frowned upon in PHD is the toxins they contain that are not destroyed by cooking. All grains, except white rice, are in this category and while some may be worse than others (modern wheat seems to be the worst by far) the others are also deprecated because in general the seeds of grasses were under severe evolutionary pressure from grass eating herbivores to protect their “babies” (seeds) from predation.
If memory serves, I may have read Paul saying that perhaps oats are the least problematic of the grains, but still best avoided strictly.
Camps of thinking that are more accepting of grains talk about soaking and long cooking or pressure cooking as means of detoxifying but if I have Paul’s view right, he considers the risk to be significant, even if reduced by these measures.
I like to eat steamed and then cooled potatoes, chopped and then warned in coconut oil as my staple safe starch, although I get the sense diversity is good and so I also enjoy yams and sweet potatoes and rice, always with fat (mostly coconut oil, or tallow, or coconut milk). Be guided by your taste. Experiment adding healthy fats until you find the ratios that are the most delicious.
Have you tried the basic pillars of the diet? A plate divided into four quarters, with near equal quantities of 1) safe starch; 2)meat, fish, eggs; 3)sweet plants (like beets, carrots, berries and fruit; 4) low cal veg (like spinach, broccoli, cauliflower, lettuce, mushroom, onions) with enough healthy fat to Make everything as delicious as possible?
For most people the recommendations end up with about 3 pounds of plant matter a day. I suspect that should do the work that oats were doing for you.
Let me also add, fermented vegetables might also play a key role in your getting better, if the problems is related to your antibiotic use disrupting your gut bacteria. I’m lucky to have a local store owned by a Korean family and one of the sisters has a kimchi business and so it is easy for me to buy delicious real kimchi (almost like homemade but easier. Can you find something similar? Also look for Bubbies pickles and sauerkraut in the refrigerated dairy section. They make live culture pickles. You can also easily make your own. Search kimchi or fermented veg.
a little bit of fermented food with each meal seems to be a good idea.
Hello Randy, thank you so much for your reply, it is most informative. I have been buying supermarket sauerkraut and a few days ago i made my own for 1st time with purple cabbage. i have put it in the fridge and in a week’s time it will be ready to eat. If any good and i feel brave I might try my own kimchi : ) thank you.
Hi Sarh, glad I was able to help.
Unless I’m misreading you, it sounds like you are trying to do the fermentation in the refrigerator. I think the fermentation needs to happen at room temperature and in the dark for a few days (3-7). I do mine in a cupboard, sitting on a plate to catch any overflow as it starts bubbling. If it is fermenting you will see bubbles forming. Once it gets to a point where it small pleasantly sour the you can refrigerate to keep it from progressing further. Search the site for fermented vegetables for more guidance.
Good luck!
Sarh, I was in a similar situation. I’ve been taking herbal anti fungals (rotating every 4 weeks), probiotics specially for gut health, and a diet that is similar to PHD. I’m doing so much better! No constipation, skin is significantly improved. I hope you feel better.
Hi Paul,
With regards to the safety of the Pfizer and Moderna mRNA vaccines for COVID-19, what red flags might you be looking out for in the coming weeks/months?
What about eggs? 🙄 ❓
3 yolks per day, ideally gently cooked, from pastured chickens if at all possible.
You can discard the whites to keep protein down and avoid issues many have with the whites, or you can eat the whites, which should always be cooked.
Yolks are one of the most nutritious foods on the planet. I think Paul suggests 5 yolks to those who are pregnant or wishing to be.
The reason for limiting to three for most is the relatively high omega-6 content.
I religiously eat 3 yolks per day, from commercially pastured chickens, and am still able to keep to the low side of the omega-6 optimum, even with 2 tablespoons of olive oil (which is also one of the higher omega-6 foods in my diet).
Eggs are an excellent source of choline, which most Americans are seriously deficient in, as well as a wealth of other nutrients.
Hi Paul,
really hope you’re able to comment on this. I’ve been seeing a functional medicine nutritionist for issues related ot fatigue, brian fog, concentration/memory issues, skin issues etc. I’ve had a copper deficinecy and apparently also iron levels that were too high.
I’ve been vegetarian and vegan in the past, plus paleo and keto.
Through the Great Plains Organic Acid Test my nutritionist also says that I have an issue with oxalate toxicity so I’m on a low oxalate diet. And I have a somewhat mild yeast/SIBO issue too.
But I always find myself very convinced by your PHD and I want to try to eat safe starches. However when I eat white rice, the low oxalate safe starch, I tend to feel almost like I’ve drank some alcohol (which I don’t do). I’m considering trying just white potatoes but these are high oxalate.
I’m wondering what you make of oxalates as an issue, and why you think I’m having this reaction to white rice?
Many thanks
Hey Paul 🙂
Do you have any opinions on covid vaccinations?
Kind regards 🙂
Lukas
I don’t think 75 g is enough protein, and you can lose muscle depending on how big you are. .7 times your weight seems about right.
Hi Paul or anybody willing to answer. I recently got the PHD book and appreciate that its focused on micronutrients not just macronutrients however I am having trouble actually balancing my macronutrient ratios. My daily calorie intake is 1600kcal and im trying to achieve a 80gcarb(20%)/60gprotein(15%)/115gfat(65%)
Currently I have 250g of either meat or fish a day however I noticed that its easy to reach protein and carbs daily intake however fat is always lacking. How can i incorporate more fat into my diet without overloading protein as meat generally uses up my daily protein intake.
I use butter, avocado and double cream which i feel like im having too much of sometimes(125g). Is this okay? what are other foods for me to incorporate to allow me to intake more fat and how much protein is do you think should be the limit?
Kind Regards,
Jordan
Hi Jordan,
1600 calories is a reduced calorie intake which is not recommended over long periods of time. If you are going to restrict calories to accelerate weight loss — note calorie restriction is not necessary for weight loss, but can accelerate it — you generally want to keep protein and carbs at normal PHD levels (600 calories carbs / 300 calories protein for a reference half-man half-woman, for a typical man that would be more like 720 calories carbs / 360 calories protein, for a petite woman closer to 500 calories carbs / 240 calories protein). Fat is adjustable because fat is how calories are stored in the body and if you have excess adipose tissue you shouldn’t need to eat any particular amount of fat. So I wouldn’t worry about how much fat you eat. Just use butter or coconut milk to flavor food to taste, eat a few egg yolks daily for nutrition, and stop there.
If you are not trying to lose weight, you should eat more.
Best, Paul
Paul,
Are your macronutrient recommendations the same for people who are 65 and older as they are for those who are younger? Or should those who are older be eating more protein relative to carbs and fat? If so, how much protein do you recommend? And how much of carbs and fat? Thank you.
Mary
I assume it still might be worthwhile to restrict pro and carbs to less than 720 calories/ 360 calories for longevity purposes?
Thanks,
Nate
Hi,
Does anybody have an updated opinion on Millet?
It’s a grain, and as Paul said, “Millet is a grain and so it is guilty until proven innocent. Grains in general are very rich in toxins, so odds are millet is no exception.”
However, it was curious to me to discover that Dr. Gundry does recommend Millet. He’s against a lot of foods with lectins, even some that everybody usually see as safe, such as squads. So it’s surprising that he says that millet indeed is safe: https://gundrymd.com/millet-lectin-free-carb/
He seem to gain this knowledge in part by having their patients test different foods with or without pressure cooking, so he says that pressure cooking can deactivate lectins e.g. in legumes, nightshades, etc., but not in wheat products.
So does anybody here have experience with Millet? Either personal experience or having read studies on it.
Thanks,
Héctor
Sorry, I meant ‘squash’, the food, not squad!
I am just starting the Perfect Health Diet, but would like to know how best to measure the “1 lb Sweet Plants, 1 lb Safe Starches, and 1 lb Vegetables” per day. Do I have to buy a scale? Are the recommended weights raw or cooked? Is there a way to say how many cups of these equal 1 lb / day? I am excited and eager to begin this healthy diet to be able to lose weight long term and follow a healthy eating plan for life. Any suggestions on this is greatly appreciated.
Hi Tawny,
You don’t need a scale. Weights of natural whole foods are all around 1 g/ml so just make the volumes of sweet plants, starches, vegetables, and meat on your plate approximately equal, and then eat to appetite, and you’ll be fine.
Best, Paul
Hi, please can you let me know if organic oat milk is safe?
Read the book and started the diets a few days ago. Doing this for arthritis and auto-immune issues. I have a question about “night-shades”. Having followed the no nightshades arthritis diet for a few years. No potatoes, tomatoes, eggplant or peppers. (Sweet potatoes not included). Just wondering if the Jaminet’s have heard of this and if I should head it still. Looking forward to the diet changes, but not sure I can consume this much food within two meals? Thank you so much for all your work and research.
Hi Rita,
Nightshade plants have toxins in their leaves and fruits, but not in underground organs like potatoes. So you can eat potatoes without fear. Most people can handle tomatoes, peppers, and eggplant just fine if their digestive tract is working well. So even if you were sensitive in the past, you may find at a future date that you have come to tolerate these. It is good to experiment from time to time, adding or removing the nightshade fruits from your diet, to see if it makes a difference.
Best, Paul
Hi Paul I’m wondering what your opinion is of the current covid vaccines?
I’ve commented above, e.g. http://perfecthealthdiet.com/the-diet/comment-page-30/#comment-1841406. There are many uncertainties around these vaccines.
Hey Paul, this quote from the book is driving me a little crazy. Are you saying on a 2000 calorie diet you should have 20 calories (1%) or 5 grams of fiber?
“Supporting evidence for the idea that 1% of energy as fiber may be just about perfect comes from clinical trials, which provide few signs that health can be improved by increases or decreases in fiber consumption.” – page 165
Hi Tama,
Fiber provides about 1.4 calories per gram, and the optimal amount of fiber is probably in the range of 15-30 g, so that would be 1-2% of energy.
Best, Paul
Thanks, Paul. American nutrition labels and nutrition apps seem to assign 4 calories to a gram of fiber.
I enjoy eating eggs and a bit of dairy (both I can obtain from a natural, organic farm directly) and yet I react poorly to them. Has anyone been able to overcome a food sensitivity or allergy to either?
Paul,
What are your thoughts about the risk of vitamin A toxicity from eating beel liver on a regular basis – even in small quantities, for instance 1/2 ounce per day?
Thank you.
Mary
He addresses this in the book in the vitamin a section. Mentioning this concern of too much vitamin a in the presence of low d and k levels.
Making sure not to supplement A and get enough vitamin d to avoid vitamin a toxicity issues.
Been following this diet pretty religiously since the beginning. At 86 I recently needed a minor surgery afterwhich a tech from the hospital lab came into my room to check me out because they had never seen a woman my age who aced all the tests and labs and took no meds or supplements. PS: I also do a quarterly five day liquids only fast.
It works folks and best part is you are never hungry.
Hi Erp what does a normal day of eating look like for you?
I can’t eat as much as Paul recommends, but I do drink lots of water.
Breakfast: rice cereal, blueberries in season, raisins when not, black coffee. Morning snack: mixed raw nuts augmented by more pistachios and apple cider (no additives, label ingredients, Apples. One meal at about 3 pm with whole milk, again no additives, no vitamins, etc.
Regular food, i.e., meat, fish, veggies, potatoes, sweet potatoes, white rice prepared in various ordinary ways, lots of butter, occasionally olive oil — can’t tolerate coconut oil. Don’t use condiments or spices very much. I like to taste the food as it is not disguised.
One square of dark chocolate everyday and there are some crackers I like that meet standards and cheese and fruit for snacks. Special treat of ice cream occasionally. Our local supermarket brand is excellent. Their Trinity features chocolate in three different manifestations. Yum!
It’s not boring and I’m never hungry. I also follow regular sleep habits, etc. — it works. I drop off immediately and sleep solid for 8 hours and sometimes even a little longer.
I hope I didn’t take up too space here. 😱
Erp,
Thank you for your post above – as a woman I am very interested in what has worked for you on the Perfect Health Diet and I think you originally lost weight for an operation? Do I have that correct – I need to lose weight and as a menopausal woman am wondering exactly where to start – any help would be appreciated.
Thank you, Paul. I have indeed noticed that China’s covid vaccines are considered ineffective and wondered why.
Less effective, not “ineffective.”
Hi Paul.
I’ve been following the PHD for a few years now. I even own several copies of the book so I can lend them to friends!
I’ve repeatedly scratched my head trying to reproduce the Fructose Fractions presented in the Safe Starches section of the book (page 100).
I’ve tried to divide the fructose by the net carbs, divide fructose by glucose, divide all sugars by net carbs, etc…
Would you be willing to reveal your general methodology?
Thanks!
What I have done is…
net = net carbohydrate grams (fiber excluded)
f = fructose grams
s = sucrose grams
I compute (post digestion)…
totalFructose = f + s / 2
totalGlucose = net – totalFructose
Since sucrose breaks down into fructose and glucose.
I make the assumption that all other carbs break down in glucose.
Finally…
fructosePercentage = 100 * totalFructose / net
This method finally produces numbers in range with those in your book. Hurray!
Hi everyone,
Does anyone have a dog that eats the PDHD, aka the Perfect Dog Health Diet? Just joking, but we could find it out.
My family surprisingly adopts a puppy in two days. I haven’t had time to plan much, what a stress! Looking at the composition of dog breast milk, and AR’s, I come up with a cheap diet that would be something like:
Per 1,000 Cal:
– 200 g 24 h fermented yogurt
– 200 g potato
– 100 g coconut milk (no sugar, no additives, emulsion of 18% fat in water)
– 100 g chicken hearts and livers (they are sold together)
– 150 g chicken feet
– 1 sardine or other fish or scraps from cleaning it
– 2 egg yolks
– Chopped eggshells on top of the food
– 2 or 3 nuts (almonds, pistachios, hazelnuts …) and fruit or vegetable peelings
And as a supplement:
– 1 dried wakame seaweed per day
– 1 tablet of 2 mg of copper bisglycinate per WEEK – not per day – but smashed and distributed in different doses – not all at once.
– Eggshells chopped on demand in a bowl (after disinfecting and drying)
– A pinch of salt per WEEK, not per day. Don’t add if your puppy will eat some human leftovers
This makes for about 65% fat (mostly saturated and monounsaturated), 25% protein, and 10% carbohydrates.
Dogs are totally weaned at about 7 weeks’ mark. As the puppy grows, you will change the natural-foods amounts approximately by:
– 2 to 3 months, 10% of its weight
– 3 to 4 months, 8% of its weight
– 5 to 6 months, 6% of its weight
– 7 to 8 months, 4% of its weight
– 9 to 10 months, 3% of its weight
– 11 to 12 months, 2% of their weight
As it grows up, their food composition may be better at about 70% fat (of which 2/3 are saturated and monounsaturated; 1/3 is unsaturated), 25% protein, and about 10% carbohydrates.
I would steam its food. I think raw food may be risky, especially organ meat and chicken. However, apparently bones must be raw to prevent harm to the dog.
—-
So,
Would this be a good plan? Is there something dangerous about the foods that I plan to feed my puppy?
So far I think it would cover all their needs (I have input all their needs on Cron-o-meter and checked it), but I’m not aware if any of these foods is harmful for them (e.g. toxicity or allergenic).
(PLEASE don’t mimic this diet, this is a very quick guess for a cheap healthy diet for puppies, and it’s risky as it’s been made with zero knowledge on dogs).
Best,
Héctor
P.S. To be precise, vitamin E would be lacking on these foods, apparently. The RA is 7.5 mg per 1,000 Cal for puppies, but these foods only provide about 3 mg.
To solve this, one could mix a tablespoon of high-oleic sunflower oil per 1,000 Cal, which would raise vitamin E to 8.4 mg/1,000 Cal.
P.S. 2: If animal foods are cooked, maybe taurine should be supplemented. I’m not sure yet. Hm, I rather make the diet simpler or I will end up dedicating more time to my dog’s diet than mine! The key is to give it foods that you eat yourself as staples, so that they don’t need much though or extra preparation.
P.S. 3: Hm, maybe it’s good to substitute that pinch of salt for a few drops of fish sauce in each meal. It would add nucleotides.
P.S. 3: Eggshells are about 95% calcium carbonate (5.5 g) so bones are better after all, as they would provide a good balance between calcium and phosphorus. Eggshells would be fine for calcium, but lacking phosphorus.
Hm, so for a solution… After cooking bone broth from thick pieces, you obtain a few pieces of bones that are pretty softened and safe. I don’t think they can break into dangerous chips, or break the dog’s teeth, and they rather break into powder and not many pieces that can produce choking. If the dog is willing to chew on that, it would provide calcium and phosphorus for free with few risks.
A mere 10 g of beef liver is super nutritious and would substitute the copper supplement. I don’t know why I didn’t include it before… I saw that the B12 allowance of puppies is 12500 IU and that was my only concern (although I don’t really think B12 is a vitamin to be afraid from if it comes from natural sources… if taken at a single meal there is no way all of it will be absorbed, and it would be stored in the liver anyway, so I can imagine that if there is a maximum allowance, it is for the very long run). So 10 g of beef liver is OK and fits perfectly (including for B12 maximum allowance).
(The dog’s a puppy yet. It’s better to kept them with their mother and siblings for 7-8 weeks, but sadly this one was taken at the 5th. So he will tolerate the traces of lactose in the yogurt as he should still be having some milk. As it grows up, I’ll be looking at the BARF diet as a reference).
Also, the coconut milk is among the most expensive ingredients and seems not to be necessary. This puppy would be licking the remains from the cartoon, but not much is needed, as they already have enough fat if you include the 10 g of high oleic sunflower oil for vitamin E. Or you could just increase the whole milk yogurt as long as they are puppies–I might be scared of growth factors, maybe the dog ends up being huge?
I have calculated about 1.30 € per 1,000 Cal. This is acceptable to me, keeping in mind that it would give it a better quality of life and would save health costs in the future. If a medium size adult dog needs about 1,400 Cal/day, it would be about 55 €/month. The real cost in this case would be lower as I get some offal for free (lungs and trachea, kidneys, etc. from lambs) and it would receive some leftovers and other rests from cleaning fishes that otherwise would have gone to the trash.
Ops, I got the value of 1,400 Cal from a very active, growing young adult dog. The actual amount seem to be more like 600 to 1000 Cal. That’s good news.
Back in the day I centered the discussion on B12; it was actually vitamin A the problem. And hypervitaminosis A can be serious. Fortunately the amounts that I detailed aren’t exceeding critical amounts.
I apologize, the first recipe was very unbalanced, e.g. it contained too much potato, had less manganese than I thought, was too rich in collagen, and lacked muscle meats.
The puppy did not suffer from its owner’s impulsivity and inexperience because I realized these mistakes before feeding him. Even so, its diet is kind of resilient as it’s given a variety of foods and can choose what to eat and what to leave.
I observed he loves beef and chicken livers, yogurt, beef, softened tendons, and egg yolks; he eats chicken breast reluctantly, and nibbles a little on softened bones and vegetables (carrots he eats well; potato eats a bit; others vegetables, barely); he doesn’t eat a bite of egg white at all. It seems like he’s choosing wisely!
Now, a representative week of foods per calorie contributions looks like:
– 6% yogurt,
– 11% chicken and beef liver,
– 2% other organs,
– 4% potato,
– 30% muscle meats (red and white meat, some fish),
– 30% collagen-rich tissues (such as chicken feet, or beef tendons),
– 9% egg yolks,
– 3 or 4 mussel meat per 1,000 Cal,
– Bone minerals; my goal is to get about 3 g of calcium from bones per 1,000 Cal (which will automatically be balanced with phosphorus). That’d be about 11 g of dry bone powder per 1,000 Cal. Actual bones have variable weight: I read that when raw they contain about 30% water, they have soluble proteins, and you have to account for tendons and meat attached, so this may translate to about 30-70 g of bones.
– Wakame seaweed (which has an intermediate amount of iodide; others such as kombu are too concentrated and are riskier because differences in nutritional analysis or mistakes committed can make a huge difference in the iodide amount). Puppies seem to need about 200 mcg of iodine per 1,000 Cal. Wakame (fresh) seems to have about 40 mcg per gram, so it would mean about 5 g per 1,000 Cal. I’m crushing the seaweed but not powdering it.
– I’m adding variable amounts of vegetables and fruit, depending on my own leftovers, and the puppy is the one to choose. He usually eats tiny bits, except for cooked carrot, which he seems to like.
– The ~10% of calories non-specified come from these vegetables and some nuts, e.g. if I’m eating almond and I drop two, I save them for the puppy.
– I’m supplementing taurine as a precaution because it’s a cooked diet–a rapid search shows that about 50% of taurine can be lost during cooking. As a reference, beef, veal, pork, or lamb contain about 40-50 mg of taurine per 100 g. So I don’t think you need to supplement much, on the order of 100 mg of taurine per 1,000 Cal should be fine. That’s also in line with what cats need.
– I’m supplementing a few drops of fish sauce per day, it apports a bit of salt and nucleotides.
—
One can do well with many different combinations of muscle, offal, and bones, and I’m choosing those because are cheaper and easier to organize for me, based on my own weekly foods. I use some yogurt and more collagen-rich material than desired as it makes it difficult to reach correct amounts of zinc.
I think the key nutrients difficult to obtain if you are not paying attention are:
– Manganese. Beef liver would be the mainstream source, but it would require too large amounts that would very much exceed cooper and B12 needs. I have heard hair is rich in manganese so maybe in nature, they would obtain some from it? The solution I found is feeding about 3-4 mussels per 1,000 Cal. I don’t feel comfortable trusting seeds as a source of manganese.
– Iodide. I use wakame seaweed (or other intermediate content algae).
– Vitamin E. There are no staple sources of animal vitamin E, so you may need some sunflower meal or sunflower high oleic oil (about 10 g either case per 1,000 Cal). An occasional almond helps too.
– Vitamin K. In this case I think cron-o-meter is not accounting for K2 in meats (I think pork can be rich on it) and yolks. I have heard dogs obtain a good part of their needs for this vitamin from bacterial fermentation in their colon; I don’t know if it’s true.
– Vitamin D. In this case most is obtained from egg yolks and occasional fish. Maybe a bit of cod liver would be a safeguard–I eat a can of it from time to time and can save bits for the puppy.
– Calcium and phosphorus. Solving this was tricky, as I’ve come to think that chewing on bones has considerable risks no matter if cooked or raw. Also, I guess dogs need that chewing work to develop correctly their jaws. So what I’m doing is crushing soft bones and adding them to its feed, and using toys to engage jaw work.
Now I feel more confident that following these guidelines (not the original that I posted) will be fine and healthy. It may not be perfect but not catastrophic either, and if it did have a fatal mistake, I hope to realize soon as I keep researching from time to time.
I prepare a week worth of food on Sunday. I thought it would require less organization, but it’s being fun and educative, I’m happy to see the puppy enjoy its food, he’s growing well, and so far he seems to be doing better than its siblings. That’s worth it.
So hope not to be taking too much space here in the comments!
Cheers,
Hector
Hi Hector, I don’t have anything to contribute unfortunately but your puppy is lucky to have such a caring family!
Thank you, Alexandra! So far, it’s going great.
I’m biased but I can see he’s growing better than its other two siblings that I know and are eating kibble. When the siblings were under 10 pounds, he was 15 pounds. Its body composition is better too–taller and more athletic. It had irritation on its tummy, presumably from pee, but while in its case it was just mild pinkish irritation, its sister had much worse irritation and developed lots of pimples over her tummy. Its temperament is also much more balanced and he learns well, and diet may help here too although genetics and socialization may be the biggest contribution here.
Regarding the diet, I’ve doubled the amount of egg yolks to apport about a 20% of calories in the diet, as they are very cheap and help with vitamin E and nutrient-dense fat. I’ve also increased the amount of omega 3; fish is cheap here and some of it ends up in the trash at the end of Saturday otherwise.
I can’t think what kibble nutrition does for dogs. Even if the kibble was made from healthy ingredients, it has two drawbacks: (1) feed requires the extrusion process, and for that a carbohydrate must gelatinize, so all feeds are very high in carbohydrate (minimum 40%); and (2) I imagine the industrial process rancidifies fatty acids and produces toxins, so even if you started from healthy raw materials, the end product would be harmful–I’ve heard dogs do not tolerate substances generated by aggressive cooking as well as humans.
If I were to use kibble, I would look for a good one (in the next contribution I will write the criteria I’ve found for choosing a decent one), and supplement it with omega 3 sources and egg yolks. I would manage it by trying to prevent mites from nesting in the feed (e.g., proper storage and not buying too much at once). I would rotate it from time to time with other brands. I would avoid ingredients such as peas and lentils, which are associated with canine dilated cardiomyopathy (DCM) in the long term, and I would opt for feed with rice or potato (rotating them).
I can think of three other solutions to kibble:
– Now there’re plenty of brands that sell BARF already made, and you can have it raw or cooked. But it’s too expensive and requires plenty of room at your freezer.
– You can also buy dehydrated feed, which is similar to kibble in convenience (although it depends on the final humidity), but again, it’s quite expensive too.
– Cans of food–I have found some decent ones for 2€/kg that are made with offal (heart, lungs, liver, belly, udders, meat byproducts).
When my puppy will be grown up or I cannot longer do batch cooking, I’ll probably give him cans, supplemented with leftovers and egg yolks, and large steamed bones that don’t splinter like hip bones for recreation and teeth cleaning.
Best,
Hector
Glad to hear it’s going well! You’re providing an extensive source of information here that is appreciated. I hope to be a puppy parent again in the future… Enjoy!
Some results for my puppy.
1. Size — He’s about a month or more ahead of his siblings in growth. That may not sound like much, but considering they are 4 months old, it is. He weighs more but is more athletic and taller. (However, it is often said “dogs on the BARF diet grow slower”. Is it a sign that the owners are doing BARF wrong?)
2. Teeth — He started shedding his teeth a month earlier than his siblings, and at a quicker rhythm. His teeth are very well positioned, except for one incisor which is slightly bent outward. Other dogs I have seen have crooked teeth.
The teeth was lost and grow in a clever choreography. First he lost the top and bottom two center incisors. When these grew in, then he lost the neighboring ones. The same for the molars: first he lost one row, and when it grew, he lost the neighboring one. The same with the tusks: the permanent upper tusk has grown right next to the milk tusk, perhaps because this way the dog is not helpless while the new one is growing.
3. Odor — His breath has a neutral odor. But curiously, when I replaced the small part of potatoes in his diet with rice, his breath did start to smell bad. My hypothesis is that some of the starch in the rice goes into the free water (I mean the water left over from boiling it) and that causes bacteria to proliferate more easily than with the potato (which has virtually no free water, I steam them).
4. Food trouble — When he eats something overcooked or a dry snack that is burnt, he gets diarrhea. This perhaps suggests that dogs tolerate new substances generated during cooking very poorly. (His diet is steamed; the cooked foods I am referring to are industrially cooked snacks: lungs or pork ears dried at 140 Celsius degrees, which sometimes have the thinner pieces burned off and seem to produce diarrhea; in other occasion, it happened with broth boiled for hours — so overcooked moist foods seem problematic too).
5. He has a very good tolerance to pain. For example, when the chip was put in, the vet asked a colleague to hold the dog so that it would not move. The needle is very thick and dogs squirm. However, he didn’t even flinch.
6. He is very relaxed about food – he doesn’t bother people, nor does he freak out every time he sees something lying on the floor. This suggests to me that the dogs I see, so obsessed with eating anything other than food, are perhaps chronically malnourished. Or perhaps ill-mannered if their owners have reinforced the behavior of begging for food.
…
Not to be biased, I should mention bad things.
7. For the past month, he has had occasional diarrhea. I don’t know why. Maybe because he is shedding his teeth? Or probably because he likes to dig and eat buried things. I have pots where I buried thinks like calf bones and avocado seeds (I did this before I knew I was getting a dog adopted; I liked watching things decompose or grow). How does he know they’re there? I don’t know, but it doesn’t seem random. Is he able to smell half-decomposed bones under a pile of dirt? It seems so. Maybe I should train him to be a police dog. The other time he found an avocado pit, which is poisonous to dogs, but he didn’t care — and a few hours later he had diarrhea. (This is in contradiction with the point 7; he has had stages in which he tried to eat leaves, sticks, dirt, and so on. I couldn’t justify this being a pica; e.g. when he started tasting dirt, which is associated to iron deficiency, I offered cooked chicken blood, but he’s not attracted to it and it’s the last thing he will eat on his plate. It seems more like learning/exploratory behavior that vanishes over time with no clear reason.)
8. He wears out his nails too quickly. Three times he has even bled because the wear reached the vascularization. I don’t really think it has much to do with food. He plays a lot with other dogs and do so by running on asphalt. Animal nails are well designed for dirt, but asphalt is very abrasive. That’s why horses wear shoes, I imagine. So I think the trouble is abrasive surfaces, not diet or others.
Correction: “6. He is very relaxed about food – he doesn’t bother people, nor does he freak out every time he sees something lying on the floor. This suggests to me that the dogs I see, so obsessed with eating anything other than
foodfeed, are perhaps chronically malnourished. Or perhaps ill-mannered if their owners have reinforced the behavior of begging for food.”Also, he regulates your appetite very well. If he is not hungry, he leaves food on his plate. On the other hand, if I see that he’s leaving the plate clean, I increase the amount of food in the next feeding. This way he is at the perfect weight without me really needing to measure anything.
…
In conclusion, I don’t think this all brings anything new. Simply put, animals eating a decent diet grow healthy. If only humans would do the same!
I just wanted to say that I bought your book yesterday and have already finished reading it. It’s the finest book I’ve ever read on diet and nutrition.
Thank you Jerry!
I have been following your diet since being diagnosed wih late stage bcell lymphoma in April 2016, after 21/2 years of rituxan nfusions, it was gone, but I belive it was more about the diet than the toxic medicine. I continue to follow it and wil for the rest of my life. I did get 2 Covid jabs due to pressure n job, but figured if I could handle those infusions and neutralise them with PHD, I could do the same with the vax. I will NOT be getting a booster, but rather trust my immune system to keep me healthy. Thank you for this incredible gift.
Dear Lynne, Great to hear about your cancer recovery, thank you for sharing! Too bad you got the jabs, but I’m glad to hear you won’t get a booster. Best, Paul
Please excuse typos – it was late and I could not find my reading glasses – I work for a newspaper,and the pressure was on – my oncologist is Chinese, and she advised me to get the Phizer jabs- I had a really bad reaction to the second shot – similar to a “flu” I caught in early 2020, leading me to believe it was in fact, COVID. I treated it with herbs and broth – and was fine. I am and have been drinking pine needle tea daily since the first jab – recommended by a doctor friend in Israel, who is also against the jabs. I truly believe after following this diet as long as I have, that food is our medicine. Thanks for responding,and for all the work you and your wife are doing.
Hi,
Paul or Eric, if you can answer, I’m super curious to know what you think about dogs, health-wise.
To sum up:
– It’s logical to think that the health benefits they provide are mainly due to force their owners do more physical activity, and provide company and love.
– Against those are, above all, the risk of zoonotic diseases–and others such as accidents, that should be greatly diminished if the dog is well educated.
So if someone follows the PHD and has already well covered the physical activity and socialization parts, how great is the infection risk and how much would it impact human-health?
I’m trying to educate my puppy to stay out of the kitchen, off the couches, out of the bedrooms, and not lick our faces. Because I suffered so much from ill-health, I’m quite afraid of infections.
Thanks,
Hector
Hey Paul! I was wondering what would be a safe temperature to cook rib eye steak in a pan? I read in the book that anything above 400 F is not healthy.
FOOD-ONLY VERSION OF PHD
This is a thread dedicated to the implementation of PHD with food only, ideally with no supplements at all (in reality, it seems vitamin D in winter and K2 may still be needed).
I suggest that each new topic be treated as replies to this opening comment, and each new topic will be developed as sub-replies to the comment it belongs.
——-
Here I will be mentioning Eric a lot. He’s a long-time user who has made excellent contributions in the comment section over the years. From reading him, it becomes obvious he has solid scientific training, well-formed judgment, and a critical spirit. It seems that in 2017 he implemented the food-only approach and made well-researched contributions to it on which we can build.
— IODINE
Hi Eric (and anyone who wants to join),
I am going to share some of what I found regarding seaweed. The goal is to know what the best seaweed for the purpose of obtaining iodine in the healthy range while minimizing risks and drawbacks.
A problem that we face is that there are too many species but too few studies. From Wikipedia: “There are about eighteen edible species in Laminariaceae and most of them, but not all, are called kombu. Confusingly, species of Laminariaceae have multiple names in biology and in fisheries science”. [Source: https://en.wikipedia.org/wiki/Kombu%5D
Another problem is that it might be that the concentration of some substances in seaweed, even at the same location and with the same growing practices, can be highly variable from year to year. Either that, or it’s an issue of taking representative samples (which in any case might mean commercial products can be very different depending on what proportions of tissue are used). From seaveg.com, “dulse bromide levels were 75 ppm in 2014 and 1,400 ppm in 2016. This is puzzling because bromine is found evenly distributed throughout the world’s oceans and concentrations don’t annually fluctuate. One would therefore expect each seaweed species to contain about the same amount every year. However, studies have shown that bromide is not evenly distributed throughout the seaweed tissue and older tissue may contain more. The annual fluctuations we observed could have been due to different proportions of the thallus (leaf or frond) being included in the sample”. [Source: https://seaveg.com/blogs/articles/bromine-bromide-bromate-seaweed%5D
Due to this, I decided to start by a general-to-specific analysis.
I will start by addressing the toxic metal (Al, Cd, Pb, As, Hg) issue.
First, is of concern the heavy metal concentration of seaweed?
Let’s take the dataset from this study as a reference, which seems to agree with the rest of the bibliography. They included 72 samples of seaweed, 8 genera in total, from Europe and Asia. [Source: https: //www.sciencedirect. com/science/article/abs/pii/S0045653520321780]
When seaweed from Europe and Asia were compared:
— Europe was found to have concentrations of As (4 vs 11 mg/kg for total arsenic; and 0,5 vs 1,7 mg/kg for inorganic arsenic), and Cd (0,1 vs. 1,2 mg/kg)
— Both were comparable in Pb (0,18 vs 0,15), and Hg (0,01 mg/kg with a SD of 0,01 only for Asia)
— Europe was worse for Al (23 with a SD of 64 vs 9 mg/kg with a SD of 9). Uranium was also analyzed; seaweed contained 0,05 vs 0,16 (mg/kg) for Europe and Asia respectively.
However, seaweed from Europe was also less rich in nutritional minerals:
— Europe seaweed had 4 times less iodine (100 with a SD of 200 vs 400 mg/kg with a SD of 1500), and in general less rich in other minerals such as Cr (0,15 vs 0,6), Fe (40 vs 80), Cu (0,5 vs 4), Zn (5 vs 20). It was richer in vanadium though (1 vs 0,5 mg/kg).
So, while seaweed from Europe has a lower concentration of toxic metals (except for Al), it also has lower concentrations of essential and trace minerals.
— That means that to obtain the same amount of iodine you would need in average 3,6 times more seaweed mass from Europe than from Asia, which means that you would end up obtaining more toxic metals (4,4 times more Pb; 3,7 times more Hg; 1,3 times more Total arsenic; 1,1 times more inorganic As; and 9,2 times more Aluminum), but 3,5 times less Cadmium.
If we look at the Provisional Tolerable Weekly Intake (PTWI) for toxic metals for adults, we find:
— For total arsenic: 0,015 mg/kg body weight
— For cadmium: 0,007 mg/kg body weight
— For lead: 0,025 mg/kg body weight
— For mercury: 0,0016 mg/kg body weight
For a 70-kg person, that would be: 1,05 mg for Total As; 0,49 mg for Cd; 1,75 for mg Pb; and 0,112 mg for Hg.
So, to get 200 mcg of iodine per day from seaweed from Europe vs Asia, you would get the following amount of toxic metals, expressed as a % of the tolerable weekly intake (this index is called “risk index”):
— Arsenic: 4,96 vs 3,81%
— Cadmium: 0,24 vs 0,85%
— Lead: 0,14 vs 0,03%
— Mercury: 0,12 vs 0,03%
I do think that the arsenic figure is worrisome; seaweed needed to obtain 200 mcg of iodine per day accounts for a tiny part of the diet, yet it would amount to 4-5% of the PTWI for arsenic.
In other studies, high cadmium concentrations have been found too (e.g., https: //pubmed. ncbi. nlm. nih. gov/24785310/, which for a consumption characterized by a 4,65% risk index for total arsenic, found a 6,74% risk index for cadmium as well).
Taking cadmium as an example (just because I have this study handy…): dietary intakes for some European countries have been estimated as being between 7 and 50% of the PTWI, with plant products contributing two-thirds of it. [Source: https: //sci-hub. mksa. top/10. 1080/19440040903532079]
Presumably, a diet rich in whole, plant and animal foods such as the PHD –not based off refined foods which I expect to be low in heavy metals just as they are low in nutrient… unless industrial processing introduced traces of toxic metals in common refined foods, which I don’t know– could lead to much higher intakes.
So, to sum it up, based on this I do see a need to select seaweed that is low in heavy metals.
Erratum:
— Europe was found to have lower concentrations of As (4 vs 11 mg/kg for total arsenic;
and0,5 vs 1,7 mg/kg for inorganic arsenic), and Cd (0,1 vs. 1,2 mg/kg)…
For a 70-kg person, that would be: 1,05 mg for Total As; 0,49 mg for Cd; 1,75 mg for
mgPb; and 0,112 mg for Hg.Seaweed is divided by three taxonomic groups: Phaeophyta (brown), Rhodophyta (red), Chlorophyta (green).
Examples are:
— Red seaweed: Dulse and Nori
— Brown seaweed: Kombu, Wakame and Sea Spaghetti
— Green seaweed: Sea Lettuce
— And you also have microalgae, for example: Spirulina platensis
—
I will base the following discussion on the dataset from the study previously discussed. [Source: https: //www.sciencedirect. com/science/article/abs/pii/S0045653520321780]
Generally speaking:
— Per unit of mass, brown seaweed is 1-2 orders of magnitude richer in iodine (average of 350 mg per kg with a SD of 1140). But its concentration of toxic metals is comparable or lower to those of red and green seaweed. So, per unit of iodine, brown seaweed offers the least heavy metals by 1 to 3 orders of magnitude.
— On the other hand, the worst case is for red seaweed, which has a concentration of iodine comparable to green seaweed (16 vs 11 mg per kg), yet about one order of magnitude more cadmium, arsenic, and uranium (but one order of magnitude less aluminium).
— Per mass unit, arsenic is highest in brown and red seaweed; cadmium is highest in red, and lead is the same for the three (I cross-checked this with another study that I don’t have handy). Mercury is low for brown and red, but data is missing in this study for green.
So with regard to toxic metals, the order for an optimization of iodine/toxic metal from best to worse is:
Brown >> green > red.
A precaution:
This analysis is too broad yet to be useful… For example, Hijiki belongs to the brown division, and yet it is the commercial algae with the most heavy metals. See: https://www.cfs.gov.hk/english/programme/programme_rafs/programme_rafs_fc_02_08.html
Regarding algae such as chlorella and spirulina, I have discarded them because they contain cell walls or lipopolysaccharides that are inflammatory. Anyways I think they contain very little iodine.
Let’s now look at the content in halogens.
I don’t know much about this topic — my basic understanding is that halogens compete with iodine when they are absorbed by the thyroid, so that an excessive accumulation of halogens other than iodine can be detrimental. So, I imagine that the important thing here is to optimize the ratio of [iodine/other halogens], especially considering bromine compounds (which I suppose is either the most abundant halogen apart from iodine, or the most harmful).
I found two studies (from 2009 [1] and 2012 [2]) that were done by the same department, and with samples from the same place (coast of Galicia, in northwestern Spain; samples came from the seaweed-based industry ALGAMAR; another brand that gathers seaweed in the zone is PORTO-MUIÑOS).
They measured the total amount of iodine and bromine, as well as their bioavailability through an in-vitro model (simulated gastric and intestinal digestion or dialysis). Both studies agree almost perfectly, but the second study also includes the analysis for specific iodine and bromine species (I-, MIT, DIT, Br-, BrO3-). They use a hyphenated anion exchange high performance liquid chromatography–inductively coupled plasma-mass spectrometry (HPLC–ICP-MS) method.
Here below, I’m writing the iodine to bromine ratio (if >1, it contains more iodine than bromine). The first number corresponds to [Total I:Total Br], the second number corresponds to [Dialyzable Br: Dialyzable I]:
— 0,17 – 0,06 – Dulse (Palmaria palmata)
— 1,04 – 0,11 – Nori (Porphyra umbilicale, Porphyra lineariss)
— 6,31 – 5,54 – Kombu (Laminaria ocholeuca, Laminaria sacharina)
— 0,43 – 0,05 – Wakame (Undaria pinnatifida)
— 0,31 – 0,03 – Sea Spaghetti (Himanthalia elongata)
— 0,12 – 0,01 – Sea Lettuce (Ulva rígida)
— 0,35 – 0,00 – Cooked seaweed (Himanthalia elongate, Saccorhiza polyschides)
— 0,00 – 0,00 – Spirulina (Spirulina platensis)
— 0,36 – 0,33 – Agar-agar (Gelidiumm Sesquipedale)
— 1,92 – 0,80 – NIES-09 Sargasso
So, the order from best to worse, considering the Dialyzable values, is:
Kombu >> NIES-09 > agar-agar > nori >> dulse > wakame > sea spaghetti > sea lettuce > cooked seaweed > spirulina.
Only kombu (Laminaria ocholeuca, Laminaria sacharina) contains more dialyzable iodine than dialyzable bromine.
—
Now, regarding iodine bioavailability, there is a study that used an in-vivo method in humans.
I can only access the summary – it seems like they found a very good bioavailability, comparable to pure supplemental forms.
I will copy what is mentioned about that study in [1].
“In this paper an in-vivo study using two seaweed: laminaria hyperborean (brown seaweed) and gracilaria verucosa (red seaweed) with high levels in iodine as a mineral or an organic form was carried out. The iodine bioavailability from gracilaria verrucosa is better than for laminaria hyperborean.
To explain these results, authors compare the possible chemical form of the iodine; in brown seaweed like laminaria, the iodine is present as a mineral form, iodide for 81–87% and an organic form for 13–19%, as residues of monoiodo-tyrosine (MIT) and di-idodotyrosine (DIT) (André, 1971). For the red seaweed, it is the reverse 35–40% of iodide and 60–65% of organic iodine with a level of MIT = DIT. To obtain these data they used a simple method to differentiate mineral and organic iodine, precipitation by trichloracetic acid (Marchal et al, 2000), around 80% of organic iodide was found in Laminaria hyperborean and in Gracilaria verrucosa. In our opinion probably this is not the most appropriate method to differenciate the chemical species in the seaweed, and a more complete method using High Performace Liquid Chromatography with an Atomic or Mass Detector must be used.
Although these results about bioavailability are higher than our results, it is not possible to perform a direct comparison because they correspond to a vivo study and our results were obtained using an in-vitro procedure. On the other hand, there are not similar studies from bromine”.
—
References
[1] https://www.researchgate.net/publication/248511206_Bioavailability_study_using_an_in-vitro_method_of_iodine_and_bromine_in_edible_seaweed
[2] https://www.researchgate.net/publication/230780873_Speciation_of_the_bio-available_iodine_and_bromine_forms_in_edible_seaweed_by_high_performance_liquid_chromatography_hyphenated_with_inductively_coupled_plasma-mass_spectrometry
[3] https://pubmed.ncbi.nlm.nih.gov/12146713/
Erratum:
“…The first number corresponds to [Total I:Total Br], the second number corresponds to
[Dialyzable Br: Dialyzable I][Dialyzable I: Dialyzable Br]:”What was found re iodine/bromine ratio seems to be a general rule: the kind of seaweed that concentrate such high amounts of iodine do not concentrate bromine in a proportional manner, thus they offer the most iodine per unit of bromine.
See abstract from [1]: “Many species of the order Laminariales (Phaeophyta) were characterized by high iodine contents: Laminaria japonica, L. cichoriodes, L. inclinatorhiza, Cymathaere japonica and Alaria marginata. The Br:I ratio for all the species except those that concentrated iodine, was more than 1”.
(Note that they are using Br:I which is the inverse of the ratio I used).
…
This was interesting too: “Seaweeds that grow at greater depths showed increased iodine and bromine contents. A tendency toward increased iodine content was observed in species growing further to the North. Iodine and bromine were accumulated selectively by various organs of Sargassum pallidum”.
—
Reference
[1] Concentration of lodine and bromine by plants in the seas of Japan and Okhotsk. https://link.springer.com/article/10.1007/BF00541002#citeas
Key points:
– Seaweed concentrate toxic metals. Of concern are arsenic and cadmium (lead, mercury, and aluminum are far from the limits set by the PTWI).
– Seaweed from Asia, compared to those from Europe, seem to concentrate more minerals per unit of mass, both nutritional and toxic.
– Per unit of iodine, however, European seaweed, compared to Asian algae, contain more toxic metals.
– Generally, it seems that there is seaweed that concentrate much more iodine than toxic metals. This seaweed usually belong to the taxonomic group Phaeophyta (brown seaweed). E.g. genera Saccharina, Laminaria, Ascophyllum, Undaria.
– Of the seaweed examined, only Kombu (Laminaria ocholeuca, Laminaria sacharina) contained considerably more iodine than bromine (by a factor of 5-6).
So, is kombu the best kind of seaweed for our purpose?
Of course, it has the disadvantage that it contains so much iodine that the amounts of seaweed needed per day are minuscule, in the order of 0.05 g.
To bypass this inconvenience, there are two ways that come to mind:
— Dilute the seaweed in another substance. For example, mix in the order of 10 g of machine-chopped kombu in 1 kg of salt.
— Use the traditional method: prepare a broth with kombu. Information on the label of dried kombu from the brand PORTO-MUIÑOS [1] (containing 309772 mcg of iodine per 100 g), shows up that a broth can be prepared with 1 g of this kombu in 1 L of water, boiled for 5 minutes, that will have a final iodine concentration of 118 mcg iodine per 100 ml.
As iodine is volatile, this procedure should be done at the final stage of the preparation of whatever broth.
—
References
[1] https://www.portomuinos.com/shop/es/algas-deshidratadas/107-kombu-desh-100-g-ecologico.html
What do you think about all this, Eric? What do you plan to do yourself — would you still favor nori?
I will be reviewing more studies in the next few days to see if what we saw here fits the general picture.
Hi Hector,
The two reasons I prefer nori are:
1. It seems easier to consistently dose. No need to measure out milligram quantities; you can just take two sheets out of a bag.
2. The amount of nori needed to provide optimal iodine intake should also provide helpful amounts of other nutrients (e.g. vanadium, magnesium, B6). I don’t think that would be the case for other seaweeds since the quantity would be so small.
For most species of seaweed, the only contaminant I would worry seriously about is cadmium (and maybe also lead).
The PWTI for arsenic is for *inorganic* arsenic exposure. But in most species of seaweed, arsenic will be present as nontoxic organoarsenic compounds. (Hijiki, which can accumulate inorganic arsenic, is likely an exception.) In fact, not only are organic arsenic compounds fairly nontoxic… they are probably a beneficial nutrient in humans. See for example https://pubmed.ncbi.nlm.nih.gov/24197927/.
Bromine toxicity from seaweed is pretty speculative… and in fact there is actually some pretty good evidence that bromine is also beneficial trace mineral. See for example https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4144415/
By contrast, lead, cadmium, and mercury, are quite toxic, and it is worth some effort to avoid them. Fortunately, seaweed always has negligible quantities of mercury. High levels of lead occur occasionally, and high levels of cadmium are more common. Generally seaweed grown in unpolluted waters (as is the case for most Korean seaweeds) will have noticeably lower levels of cadmium than seaweed grown in polluted waters (as is the case for many Chinese seaweeds).
Best,
-Eric
Hi Eric,
Thank you! Having your feedback is always enlightening.
Yes, I figured you also used nori as a source of nutrients, which is an aspect that is lost when using kombu.
Also, the in vitro studies I’ve seen tend to give implausible iodine digestibility — too low. The only in-vivo study I’ve found had much higher results. So, probably its I/Br ratio is closer to 1 (better than most seaweeds). Then, if you tell me that bromine isn’t to fear in trace amounts, I may embrace nori too!
Finally, there’s something about eating with seaweed sheets that sounds appealing… Maybe I’ll even dip it in the egg yolks — anyway one can’t get much weirder; the point at which I crossed the barrier of wearing red goggles covered with duct tape already exceeded the point of diminishing returns, time ago.
Tomorrow or so I’ll be posting my implementation of the food-only version, and I’ll try to start a discussion of vitamin C.
Best,
Héctor
Hi Paul,
Do you tend to agree with Eric regarding the bromine topic?
E.g., is there evidence suggesting that bromine concentrations are higher nowadays, compared to old times, so that we should favor seaweed richer in iodine than bromine? Is there something in your opinion we are not aware of or underestimating?
I’m asking because in the book bromine is mentioned a couple of times as a toxin; and anecdotally one can hear of people reporting bromine toxicity more than one would expect.
The official sources I found in a quick search talk about acute exposures from industrial settings. Then, this webpage [1] says:
– Many pesticides used in agriculture are known to contain methyl bromide.
– Bromine is extensively used in the manufacture of plastic, computer boards and upholstery.
– Trace amounts of bromine are often present in some flour and baked foods.
– Many soft drinks like gatorade, mountain dew, fresca and other citrus flavored colas are known to contain bromide
– Bromine is often found in certain medications like inhalers, nasal sprays and certain gaseous anesthetics.
– Bromine in the form of polybromo diphenyl ethers is used as a fire retardant in carpets fabrics, mattresses and upholstery.
– Bromine is often used for treatment of swimming pools and hot tubs.
—
Reference
[1] http://www.drcraig-chiropractor.com/blog/74692-bromine-how-is-it-affecting-my-health_2
Hi Hector, I’m by no means an expert on this topic, but my understanding is that bromine toxicity is mainly a concern in the case of iodine deficiency, and if you are getting an abundance of iodine from e.g. nori and some seafood, then there is minimal risk from bromine. The iodine will outcompete the bromine and the excess bromine will be excreted.
Best, Paul
Also: I wonder if this case is similar to that of inorganic and organic arsenic — i.e. are the forms of bromine found in seaweed or food more benign than those that supposedly come to us from pollution? Are you aware of that, Eric?
How complicated our world is. 😯
Thank you, Paul! That adds the further context I needed.
(My above comment was sent before I read your answer.)
Hello Paul, I have a burning throat issue with no type of reflux. This has been confirmed via many tests (ph and others). I have experimented with different diets. When on carnivore diet, my sleep and overall body pain gets better, but throat gets worse. When on perfect health type diet, my throat gets a bit better, but i get more cravings and a bit more pain elsewhere. The whole mucin production thing seems to make sense as a possible reason my throat gets better. I just have to do a very non acidic version of your diet to keep from irritating the throat further.
Thanks allot for your time,
Jesse
Hi Jesse, sounds like you have a small intestinal bacterial overgrowth or intestinal bacteria dysbiosis that leads to inflammation when you eat carbs, but you need the carb nutrition for mucosal and epithelial health and feel it in your throat when it is missing.
For the intestinal dysbiosis, make sure you get optimal vitamin A and D, taurine in the morning and glycine in the evening, circadian rhythm entrainment, vitamin C and egg yolks daily. Try to eat more extracellular matrix.
Best, Paul
While the Perfect Health Diet sounds good to me (and I’m coming to it after being Ketogenic with some fasting for about 3 months now), I’m not sure about the logic of assuming that our ancestors were optimally healthy on a Paleo diet. After all, plenty of people on obviously unhealthy diets these days are succeeding in having children who themselves survive long enough to reproduce; our ancestors similarly would have needed only to be healthy enough to have offspring and raise them long enough to be able to survive, which back then probably meant to about 7 – 12 years of age, given that they lived in a tribe and 7 year old orphans could have gathered food like the women, and 12 year olds would have been ready to join the males in the hunt.
Hi Mark,
Two comments:
– It would be more helpful to think in terms of diet-genome co-evolution, along the same lines as gene-culture co-evolution. Natural whole foods were the only foods available and so we evolved to fit a natural whole foods diet. “Paleo” essentially means natural whole foods. Our bodies are maladapted to diets our ancestors never ate nor could have eaten.
– It is a mistake to think that evolution only selects for fertility, or ability to reproduce. In our ancestral environment low-level warfare was incessant and 30% of men died from homicide. If you weren’t successful in warfare, you wouldn’t reproduce. Who is going to be more successful in an MMA fight, someone eating natural whole foods or someone eating Doritos and Coca-Cola?
Best, Paul
Also, only ~5 species are known to have menopause (i.e., they live well beyond their fertile period.).
So above a certain age in females, the dangers of pregnancy outweigh the benefits. This implies benefits must exist*; the mother who is no longer fertile improves the chances of her offspring surviving and reproducing. This could have been so relevant that it may have selected for longer life expectancy; see the grandmother’s hypothesis: https://en.wikipedia.org/wiki/Grandmother_hypothesis
* The other possibilities would have been that either menopause didn’t exist, so that women could have offspring all her life, albeit with few successes at old ages (and in social beings such as humans, this could hinder the whole tribe); or the mother would die at younger ages and thus would not be in competition for the resources of her offspring.
I have read however that when an older person hindered others, they were left to die, or killed. It is difficult to disentangle the interactions between genes and culture, but the fact that menopause is so rare in nature is striking.
Wondering about the possibility of using buckwheat instead of rice. Would it have antinutrients? I believe its a low glycemic carb otherwise, with some fiber.
Hi Mark,
Buckwheat is fine.
Yikes, I just saw a youtube video by Dr. Paul Mason (low carb down under) where he says that Omega3 is also a polyunsaturated fat, which oxidizes when stored and thus consuming fish oils is not a good idea. If that’s true then canned or packaged Salmon, Sardines, and Anchovies , which I rely on for my Omega3’s, are surely also suspect. Where then am I to get my Omega3’s? Should I instead focus on making sure I never consume Omega6 (i..e. no chicken ever, no turkey when I visit my relatives at Thanksgiving)? I am not in a position to catch fresh fish from the ocean.
Not sure you want links posted here, but here is the source for these claims:
https://m.youtube.com/watch?v=J_xu2zLlQAs
in case you missed it;
http://perfecthealthdiet.com/2010/06/fish-not-fish-oil-capsules/
Darrin,
Thanks. Yeah I hadn’t seen that yet – took the shortcut of asking the question instead. In fact I haven’t purchased the book yet, although I intend to do so soon. In the meantime I had arrived at what I think are most of the same conclusions, only without good evidence to back them up.
Parenthetically, most of my learning seems to operate this way. I have to somehow arrive at almost the right idea before finding someone who has said it more clearly and precisely … because otherwise I won’t be asking the right questions or searching the right topic areas.
(Hi Paul,
I wrote a comment here that has disappeared. May it be the SPAM filter? It contained a single URL to your own blog. I didn’t save a copy of the comment this time, oops.
Best,
Héctor)
Hi Mark,
— You need very little omega 3 to be healthy; about 0,5 kg of fatty fish per week does it. That may help.
— Even so, the case of fish cans is better than that of capsules. So if it’s your only option, I think you’d rather accept a bit of rancid fat if that prevents an omega 3 deficiency. Avoid those that come in unhealthy oils (seed oils such as cottonseed, canola, corn, sunflower, etc.); avoid those that have been stored for more than probably 3-4 months (the less time, the better), and perhaps avoid those that come in brine (it seems that salt accelerates the oxidation of fats). You may store the cans in the fridge (although if you store them for a long time, I’m not sure if the moist would corrode them).
— Yes, you do need to limit omega 6 as seed oils and industrially-raised animal foods are too high in omega 6. The goal is to get it under about 8 g per day, or 4% of calories. You can check PHD’s prescriptions to achieve that (e.g., avoid relying on seeds as a source of calories, avoid unhealthy oils, favor naturally-raised animals if possible, favor seafood and ruminants meats over pork and chicken, etc.).
— Being happy also promotes health, and I would not go to the extent of avoiding sharing a meal at Christmas. You can avoid the fat that is released on the tray, and avoid eating the fatty parts of the bird; or alternatively, you can purpose to have duck for dinner… Or just enjoy the dinner as it is, which would have little impact on your omega-6 balance throughout the year 🙂
Best,
Héctor
Suggesting duck is a wonderful idea. My brother (whose family I will be visiting) is an avid hunter, and while he won’t be hunting any duck, he will likely be open to the idea of having duck, and it will still seem like a traditional (more or less) Thanksgiving meal.
Heh, just like “Chinese turkey” in the movie “A Christmas Story” … It’s smiling at me …
Thanks!
That’s great! Who knows if you will end up improving the health of your relatives as well. I wish you great success and health in this new endeavor.
Hi,
This is to share how I have implemented the food-only version of PHD (i.e. the PHD with as few supplements as possible). Any feedback is very welcome.
—
The following list is intended to be indicative, as I will favor some foods or others or alter proportions according to my appetite or preference.
Here is my weekly shopping list per person (by raw weight unless otherwise specified):
– 3-4 kg of white potatoes. About 2-3 times a week I will substitute potatoes with: chestnuts, sweet potatoes, yucca, plantain, or tigernuts
– 1.5 kg of leafy vegetables (e.g. lettuce, kale, spinach, chard, endive, broccoli, brussels sprouts, cabbage)
– 1.5 kg of vegetables in season –other than leaves and greens– (e.g. onions, zucchini, cauliflower, peas, green beans, celery, radish, parsnip, leeks, turnip, artichokes, garlic)
– 3 kg of sweet plants, including 1 kg of frozen black currants and 750 g of frozen strawberries or mixed berries; the rest is for seasonal fruits, beets, and carrots
– 4-5 avocados totaling about 500 g of pulp
– 125 g of macadamia nuts (or 1 packet); about 140 g of other assorted nuts
– 1 kg of assorted mushrooms; most of the time I’ll buy them frozen
– 1/3 kg oily fish (e.g. frozen chum salmon, mackerel, sardines)
– 1 kg or so of chicken feet to make broth
– 2 dozen eggs
– 1/4 kg chicken livers
– 1/2 kg of bivalve meat, except oysters (e.g. mussels, clams, cockles, scallops) – depending on whether they are large mussels or clams with thick shells, I think this would be equivalent to 1-2 kg of raw bivalves
– 1/4 kg of octopus if cooked; 1/2 kg if raw
– 1 L of coconut cream (18% fat, no sugar added)
– Oysters: 5-7 medium oysters per week (European oysters; Atlantic oysters would be even better, but not Pacific)
– Replenish the pantry as needed: Nori sheets (to use 2 per day), herbs and spices, vinegar, extra virgin olive oil, sea salt without added iodine, dried chestnuts and tiger nuts (just because I enjoy them)
—
A few notes to clarify which choices are personal:
— I am purposely avoiding red meat, but a little kidney a week would be very helpful for selenium — so I had to substitute it for octopus
— I have a sensitivity to nightshades (except potatoes), so I’m not including red peppers, which would be very helpful for vitamin C
— For availability or limited budget, I’m not including interesting foods such as guavas or taro.
— Also due to availability or limited budget, I’m including some frozen foods (mushrooms, spinach or endives, black currants, salmon). But I think this could also be beneficial, as I will discuss in the following comments to this thread.
— For variety and personal taste, I’m including some tigernuts or chestnuts, although they aren’t as nutritionally dense.
— I don’t tolerate any dairy; otherwise, old cheese would be a wonderful inclusion to incorporate vitamin K2, calcium, and more fat.
(I am hopeful that I will eventually get better and be able to tolerate those foods that I now have to exclude). 😛
Now, let’s see how it fits in Cron-o-meter — note that I have changed the goals for nutritional values following Eric’s influence, see: http://perfecthealthdiet.com/the-diet/comment-page-27/#comment-1766291
See this picture in which I have approximately averaged a week of foods:
https://i.imgur.com/Fk6ghRz.png
—
Some notes:
— The chicken feet are to make broth and remove the fat; so omega 6 would average ~8 g per day, not 10.5 g.
— I will buy some green leaves frozen. Since folate in frozen vegetables is unstable, that should lower the folate figure about 5-20 net percent, depending on how many months the product was stored — the latter is only my guess.
— There are a few other things to take into account, e.g. I’ll cook some green leaves, specially kale (it’s rough!), and I’ll sauté the mushrooms as I don’t like them boiled or steamed. I guess this will lower the amount of B-vitamins and vitamin C.
— The black currants are listed to have 181 mg of vitamin C, but most commercial varieties seem to have lower values, around 140 mg.
Now, I’ll have to check essential nutrients that don’t appear in cron-o-meter.
So far, I know I need to optimize vitamin k2.
Three egg yolks seem to contain about 15 mcg of vitamin K2; 250 g of chicken liver per week average 5 mcg of vitamin K2. I don’t think any other food in the list will provide more than trace amounts. Homemade fermented vegetables might contain some.
So if my goal is at least 100 mcg of vitamin K2 per day (200 mcg may be better), I need to obtain at least ~80 mcg more per day!
The great help that Eric found is duck eggs, which he stated seem to consistently contain 1 mcg of K2 per gram, plus some old cheese.
I can’t get those, so I’ll check the K2-database that Chris Masterjohn created (https://chrismasterjohnphd.com/blog/2016/12/09/the-ultimate-vitamin-k2-resource) and see what could be done. But I think vitamin K2 supplements will be required here.
see Natto for K2.
It’s an acquired taste 😉
Hi Darrin,
Thank you for the suggestion! Indeed, natto seems to be approved by Paul (see: http://www.perfecthealthdiet.com/) but I’m hesitant to try it because I suffer from many food sensitivities, and soy (even if fermented) could be a candidate for trouble.
By the way, in that same discussion that I linked to, the commenter min said that K2 supplements produced heart palpitations. This might add to the suspicion towards supplements (cc: Eric).
What I find strange is that vitamin K2 is apparently so rare to find. The fact that it is an essential nutrient denotes that it should be relatively easy to find (or would have been in ancient times) in natural foods.
That makes me wonder if vitamin K2 is produced by many bacteria, and in which case, how much may be in homemade fermented vegetables. In case these were very bacteria-dependent, I wonder if I could use a bit of old cheese –from the varieties that are very rich in vitamin K2– to help the correct bacteria develop in my fermented vegetables? If it is very substrate-dependetn, then this may be useless.
On the other hand, if I recall well, the meat of some mammals is rich in MK-4, so maybe that’s another explanation.
Finally, shouldn’t a healthy microbiota produce some amount as well? But I guess the figure of 100 mcg (ideally 200 mcg) of vitamin K2 per day already accounts for that approximately.
Best,
Héctor
Hi, this is the correct link:
http://perfecthealthdiet.com/recommended-supplements/comment-page-20/#comment-118861
Hi, Eric and Paul (and anyone else),
If you had time to chime in, I’d be appreciative of your feedback.
Apart from all the optimization work that I still must tweak, I have two concerns:
FIRST:
The issue of nutrients lost in modern foods. To sum this view, I cite what Stephan wrote in a nice article [1]:
“The unfortunate fact is that micronutrient levels have declined substantially over the course of the 20th century, even in whole foods. Dr. Donald R. Davis has documented the substantial decline in copper and other micronutrients in American foods over the second half of the last century. An even more marked decrease has occurred in the UK, with similar trends worldwide. On average, the copper content of vegetables in the UK has declined 76 percent since 1940. Most of the decrease has taken place since 1978. Fruits are down 20 percent and meats are down 24 percent.”
I know Paul and many other mentioned this issue too. On this blog, Paul wrote: “We also recommend augmenting the diet with certain supplements. […] These nutrients are deficient in modern diets due to removal of minerals from drinking water by treatment, depletion of minerals from soil by agriculture, or modern lifestyles that deprive us of vitamin D by indoor living”.
So, have you looked at this and reached any conclusion, Eric? E.g. do you suspect of any supplement that still might be beneficial (apart from D3 in winter and K2 in my case) even if on paper you are obtaining all the essential nutrients?
Pardon the question;, I do understand that you have optimized your diet so much that there is little more you can do on your part… Once we did what is up to us as best as we could, the thing left is accepting the rest.
So far, I see that favoring nutrient-dense animal foods –especially seafood– to obtain as much key nutrients as possible may be a wise decision, not only because those are less likely to contain toxins, but also because I would guess that those are less subjected to nutrient variations than plants. E.g. oceans concentration is homogenized and its variations should be minimal, apart from pollution in areas of human activity.
(It may be worth mentioning that copper is usually mentioned as the most affected nutrient (we don’t know about the others?), but if anything in the food-only approach copper it’s easier to be overdosed than the opposite).
SECOND:
The optimization of all the nutrients with only-foods requires some to be in higher amounts than strictly needed. Is this trouble with regard to opportunistic infections? The regular PHD does better here.
E.g. I have trouble to get folate lower than 900%, or iron below 300%. I understand the concept of “healthiest range” for nutrients (a range in which our body can manage excesses without health repercussions for the metabolism, so low and above this range health begins to deteriorate); but does that accounts for opportunistic infections taking advantage of nutrients in amounts strictly over what we need?
—
Reference
[1] http://wholehealthsource.blogspot.com/2010/04/copper-in-food.html
Hi Hector,
Cron-o-meter primarily uses data from the newest editions of the USDA and NCCDB databases. These databases are based on recent measurements of nutrient content, not on measurements from 1940.
For people who have calculated that their diet contains enough of every essential nutrient, then as a rule, I don’t think supplements are helpful. The most likely exceptions to this rule would be:
0. Anything your calculations show you aren’t getting enough of, such as K2 in your case. By the way, you can easily find combination D/K2 supplements.
1. Vitamins C and B12 — because needs can be highly elevated in certain pathologies. I would test these. Optimal plasma vitamin C levels are 1.1 mg/dL = 60 mmol/L or higher. Methylmalonic acid (an inverse marker for B12) should be in the lab-provided reference range, preferably in the middle or near the bottom.
2. Vitamin D, lithium, silicon, and boron — because the main source is not diet, it is sunshine for vitamin D and drinking water for the other three. By the way, especially since you are in Europe, I should mention that Rozana mineral water (from Auvergne France) is very rich in lithium, silicon, and boron. Drinking just 1/3 liter per day would optimize intake of all three. I would test vitamin D. Optimal 25-OHD is between 30 ng/mL (for racial groups with low ancestral dairy consumption) and 40 ng/mL (for racial groups with high ancestral dairy consumption such as Europeans).
3. Selenium — because nutritional databases are a poor guide due to extreme natural geographic variation. Seafood is likely to be less variable, as you point out, so testing might not be necessary if that is your main source. If you do test, optimal plasma selenium levels are 90 mcg/L or higher.
4. Iron — because of extreme natural variation in the genetics of iron absorption and transport. Optimal iron saturation is 30–40%. Optimal ferritin is 50–150 mcg/L. I would measure both. Excess iron can be managed with blood donation.
Extrapolating from breast milk would suggest optimal folate intake is about 750 mcg/day. Your intake of folate is not far from this, and I doubt it is cause for concern.
Best,
-Eric
P.S.: Any testing you do should be done, at minimum, several months after your diet is stable.
Some other food databases for anyone interested.
These contain some items/foods that are not found in the US databases. So can be worth checking sometimes. Also interesting to compare the data.
Finland:
https://fineli.fi/fineli/en/index
Denmark:
https://frida.fooddata.dk/index.php?lang=en
Australia:
https://www.foodstandards.gov.au/science/monitoringnutrients/afcd/Pages/default.aspx
Hi Darrin,
That’s a great idea; I’ll do that, and if I find relevant differences, I will share them here.
To find more of these local databases for European countries, I’ve found this list: http://www.fao.org/infoods/infoods/tables-and-databases/europe/en/
I think https://nutritiondata.self.com/ is well-known, and certainly it is great and has many useful tools.
Also, recently I discovered http://www.checkyourfood.com, which combines data from several sources (see: https://www.checkyourfood.com/pages/guidelines) and allows searching for specific nutrients too.
Best,
Héctor
Bitelog is good for doing side by side comparisons of multiple foods.
http://www.bitelog.com/mega-food-search.htm
(ignore the ads)
Hi Eric,
Great information; thank you! I’ll put this into practice. I’ll report any interesting experience in the future.
“…not on measurements from 1940.” — you made me laugh. Just this once: hurray, USDA!
A few miscellaneous comments:
— For the case of chronic diseases for which it isn’t allowed to donate blood, I wonder what to do about iron overload. This isn’t my concern as my iron levels are very low; just a curiosity. I guess one should act before it is too late by adjusting the amount of iron in the diet, and maybe work around dietary factors that decrease iron absorption (which I guess is not very feasible, as such factors may affect other minerals as well).
— When I pointed at folate and iron, I meant all these nutrients that could be beneficial to pathogens — I think another example is niacin. But never mind, I realized my question was unfair: I’ve briefly re-read the pertinent characters of the book and realized that no upper limit was suggested for such nutrients; it is just said to avoid supplementing it as a rule. They also say a typical value for niacin for the regular PHD is 30 mg, the same I got for my planning. So, this “issue” isn’t exclusive to the food-only version, which implies both Paul and you agree that this isn’t a problem – in your case, you did estimate upper limits, which is a useful guide!
— If you feel like detailing on this, I’m quite curious as to how you did the milk extrapolation, as it doesn’t seem entirely trivial. Have you used the average weight of a newborn to factor each nutrient need to the adult weight, maybe to the power of 0.7 or so? Or have you extrapolated based on calories? Then, there’s a bunch of considerations that would make a book. E.g., that tissue proportions are different in children (they have a big head), or that certain nutrients may be needed in proportionately greater amounts for growth, but not for tissue maintenance; etc. I wonder how you managed this estimation or deductive work – I may learn a few things.
— Finally, I can’t help but wonder if you reached similar proportions in your diet –- what are our most relevant differences? (Today I’ve decided I will double either the number of macadamia nuts -–I buy them in 125 g packets– or the amount of coconut milk –-I buy it in bricks of 1 L with 18% fat– to increase dietary fat; and I would add 250 g of fresh mushrooms to the 1 kg of frozen mixed mushrooms in order to further increase the B-vitamins).
Best,
Héctor
Hi,
Regarding iron overload for those that cannot donate blood, these are the conclusions I reached — I haven’t dedicated much time but I hope this is approximately correct:
1. Unless you had a genetic predisposition to accumulate too much iron, you probably don’t need to worry about iron-rich foods. The absorption of heme-iron (the main form of iron in the diet unless one is a vegetarian) is influenced by iron status with an inverse relationship.
2. You can guess if you have such genetic predisposition by looking at previous blood test and whether you have tended you have high iron levels in absence of certain diseases; for women, take into account lactation and menstruation which increase the loss of iron. Or have a genetic test such as 23andMe and see how many copies you have of the allele A in C282Y (AA would be the severest risk); or the allele G in H63D (GG would be moderate risk) – there must be more gens that influence iron accumulation, but these seem to be the most relevant.
3. In case that you do have a predisposition to iron overload, the single best solution, as Paul says in the book and Eric said above, is to donate blood. About 90% of the iron is in our blood, but this isn’t true for the rest of minerals. For people who cannot donate blood, there is a procedure called phlebotomy (but I think most doctors won’t approve it until the problem is quite serious).
4. The second thing that can be done is through diet; but this is more a help than a solution, as managing or preventing iron overload through diet is not very feasible — any healthy diet will be rich in iron because it is usually paired with other minerals. So, if you can donate blood or your doctors approves phlebotomy, then there is generally no purpose to change your diet.
5. Diet-wise, you can favor foods with a high ratio of minerals/iron. For example: liver has a high level of iron, but also a high level of other nutrients, so a bit of liver per week will make your diet nutritious but not iron rich. Meat however is proportionally richer in iron than in other minerals and can be substituted by fish or bivalves (except cockles, which are exceptionally rich in iron). The rest of the calories that are derived from vegetables, tubers, eggs and nuts are not a problem.
6. The other factor diet-wise is to pay attention to inhibitory and enhancing factors. Non-heme iron absorption is enhanced by ascorbic acid, meat, fish, and poultry in the same meal, while heme iron mainly depends on the absence of inhibiting factors, and the iron status with an inverse relationship. Inhibiting factors are phytic acid, calcium (300 mg per meal may be best, as the inhibition is saturated at that amount), polyphenols such as catechol groups, e.g. catechin, or galloyl groups, e.g. gallic acid, which are found in: tea, coffee, cocoa, red wine, many vegetables e.g. spinach, and herbs and spices such as oregano and cinnamon. All the named foods have proven inhibitory effects on iron absorption at least in-vitro – e.g. 1 cup of coffee is estimated to have a 40% inhibition on iron if consumed in the same meal; a cup of tea, around 60-70%.
7. But here it is why this approach is not very useful. First, many factors inhibiting iron will also inhibit other minerals such as zinc. Second, the absorption enhancing factors can overcome the inhibiting factors in good part.
8. In exceptional cases, as a last resort, it may be worth it to explore if one could effectively separate certain nutrients from iron in order to inhibit iron absorption while not affecting so much the other minerals. I have not researched this, but take this example to illustrate the idea: oysters are so rich in zinc that you could get all your weekly needs with a meal of ~200-300 g of their meat (Eastern oysters, raw weight) – which means that you could include inhibitory factors in the meals that are rich iron, but not when eating oysters.
9. In any case, measuring iron levels from time to time is good advice.
Best,
Hector
Hi Hector,
For folate, I just extrapolated proportional to body weight.
The most significant difference is probably that I don’t eat so many shellfish (just Atlantic oysters and scallops). These are replaced in my diet with dairy (mostly Jarlsberg cheese) and additional organ meats (such as beef heart and veal kidney). By the way, you might want to look into heavy metal concentrations, primarily lead and cadmium, in the other shellfish you eat. To be clear, I’m not saying it is an issue, just that I don’t know, and I would research it more myself if shellfish were a larger portion of my diet. I only know about the pattern of heavy metals in oysters available in the US (Atlantic vs Pacific) and in scallops (it is not a concern).
Other differences are pretty minor, for example I don’t avoid nightshade vegetables such as peppers, and eat duck egg yolks in place of chicken egg yolks.
Best
-Eric
Hi Hector,
Most of your iron strategies sound okay for someone who can’t donate blood. But let me point out that zinc absorption declines significantly as a function of dose. Eating all of your oysters for the week may be problematic.
Best,
-Eric
Hi Eric,
Thank you! I envy the Jarlsberg cheese.
I will be sure to check the content of toxic metals in mushrooms and bivalves and post about it. For wild mushrooms, it’s astronomical.
Best,
Hector
Hi, I thought it might be interesting to register and share my experiences in the food-only version.
Foods I’m craving the most: nori and salads.
— I eat nori seaweed as it comes out of the package. These have close to zero sodium and are delicious. I really can’t get enough of them. I should eat about 2 or 3, but I’m eating about 5 or 6 a day — and I limit myself, otherwise I might eat a lot more.
— I prepare a big salad with fresh leaves, avocado, egg yolks, tigernut crumbles or sometimes seeds, coconut milk, balsamic vinegar (raspberry vinegar or grape must vinegar), and a dash of salt. Sometimes I add some protein source to it. I will gradually dispense with the sweet vinegar in order to reduce the fructose content, but for the moment I like it too much like this.
Foods I crave somewhat: potatoes, mushrooms, strawberries.
— Potatoes are very satisfying, but I can’t have them steamed or boiled in the broth – they’re too bland and satiate too much. What I usually do Is to steam them but then pass them to the oven to dry them a bit at about 160-170ºC, and eat them with some salt.
— Something similar happens to me with mushrooms, but even more intensely — boiled or steamed mushrooms are straight disgusting, but if sautéed with a little garlic and oil until they have lose weight, they are delicious.
— I enjoy strawberries and I miss them whey I run out of them. This doesn’t happen with other fruits, which I also enjoy but do not miss.
Foods that I like but don’t crave: Broths made from extracellular matter (I use chicken feet), and chicken livers (I make a pâté with it).
— To be fair, both the broth and the pâté are delicious when well-seasoned and I do enjoy them. But I could go every day without having or missing them.
New foods that I do not like: black currants.
— I really like acidic flavors, but these berries are *too* sour to eat by themselves or with coconut milk. I will try mixing them with other fruits or nuts.
Foods I used to crave and no longer do: chickpeas, large amounts of fruits and nuts.
— Now I’m happy with a moderate (per PHD recommendations) amount of fruit and nuts. I don’t crave chickpeas anymore — but I’m sure I would still enjoy them.
I must note that it’s very hot here and that must be influencing my taste too: a warm broth is unappetizing, whereas I fantasize about huge fresh salads.
Protein foods, surprisingly, don’t appeal to me much. Only occasionally if I eat nothing in a day, but without a marked preference toward any one source. I won’t comment much here because I haven’t implemented this aspect of the diet yet — I’m still investigating bivalves, and still couldn’t get oysters. For now, I find mussels (especially greenshells’) delicious as well.
…
As a curiosity, the biggest craving I remember in my life is when I was recovering from an illness in which I was dying, with a BMI below 16 for two years. The craving was for canned foie gras. I remember for a few weeks I needed to eat at least one can a day (about 900 Cal), and I would finish it in one meal. If they weren’t so expensive I could have eaten two or more each day. There were other high-calorie foods available, such as nut butters, but I didn’t feel as much attraction to them. Before long (I don’t think much more than two weeks) my craving went down, and it was only occasional. Today I still enjoy it, although I don’t buy it because of its production method — to be fair, I don’t know if it’s justified, since migratory birds can store fat in their livers naturally (they are not necessarily diseased), and I don’t think e.g. chickens or laying hens have much better lives in their industrial production methods – force-feeding is the last step and lasts 2 weeks.
By the way, of course my expectation is that my tastes will change over time as they are overridden.
In this regard, I find the experience of the famously infamous Theodore Kaczynski or UNABOMBER interesting. He is one of the few cases I know of in which a man raised in civilization returns to natural life in the woods, so to speak. I will quote some of his answers in an interview by J. Alienus Rychalski.
When asked “What was your favorite wild food?” he answered: “Probably the tastiest wild food in the Lincoln area is partridge berries, a tiny species of Vaccinium–the blueberry genus–that grows at high altitudes. The berries are so tiny that it may take an hour to pick a cupful, but the flavor is superb. Apart from those, my favorite foods are huckleberries, yampa, and the livers of deer, snowshoe rabbit, and porcupines”.
When asked “did you have any favorite meals that you prepared?”, he answered: “I didn’t have any standard meals, since I just ate what was available at a given time. Generally speaking, my best meals were the stews that contained meat, vegetables, and some starchy food such as potatoes, rice, noodles, or roots such as yampa”.
There are many other interesting parts in the interview.
Best,
Hector
Perhaps I should clarify that he kept a pantry with some staple foods: whole and white wheat flour, oil, sugar, and rice; powdered milk, perhaps oatmeal and cornmeal–and from here will also come the noodles he mentions.
Hi Hector, I find your contributions really interesting and some of your food choices have inspired me to experiment. I was really slacking on the chicken liver pate and am now eating nori sheets. Your salad sounds delicious. Thanks for sharing!
Thank you, Alexandra! I realize gratitude is powerful — you make me want to live up to your expectations. 😀
Please let me know how much you like nori sheets. It seems to be an acquired taste for many people.
Hi Hector, I like them more than when I tried a few years ago. Now I find myself starting to crave them. The ones I got have a little sea salt. Also good crumpled up on foods or used as a mini wrap. A larger sushi nori sheet would also work with a variety of fillings… if you ever get tired of eating them straight out of the package. 😎
Hi Alexandra, interesting that you are also starting to crave them.
By the way, these are the ones I buy, which are available in other countries as well via Amazon:
https://www.amazon.es/gp/product/B07VHD8MVY/ref=ox_sc_act_title_3?smid=AFC7ZKRHS4T2V&psc=1
I don’t know how good they are, but definitely they taste nice to me. I bought them because they are from Dadohaehaesang National Park in South Korea, which is said to have very clean waters.
…
I have had a few other experiences.
Eggs:
I bough duck-, chicken-, and quail eggs from a local producer. I did a tasting. The quail and chicken eggs had yellow yolks, the duck eggs had bright orange yolks. The quail and duck ones tasted great, and I wouldn’t be able to say which one I liked most, although the duck ones had a kind of weird flavor, like if they tasted too strongly of egg or bird–I can’t put it better–but that was not necessarily a bad thing. Then, he chicken ones were the worst in comparison–they didn’t appear as tasty to me.
(I am ecstatic to have found a local supplier of duck eggs at only 3€ a dozen… The second best price I had found was 10€ a dozen! These eggs are the same size as chicken eggs, but their yolks weigh exactly 50% more. In other words, three chicken yolks are equivalent to two duck yolks).
Sources of fat, coconut milk and macadamia nuts:
If I go a while without eating macadamia nuts (let’s say a week), they taste delicious to me–creamy, buttery and nutty. But if I eat them more often, they taste insipid. However, coconut milk–which is my other main source of fat, apart from whole foods–tastes good to me every day or even several times a day. Whether in salads, with strawberries, or in sauces. I even sometimes like to have a few spoonfuls without anything else.
Nuts:
In the pantry I currently have almonds, cashews, Brazil nuts, macadamia nuts, walnuts, pecans, pistachios, hazelnuts, pine nuts… But, although I don’t have a strong craving, I do tend to always resort to almonds. Cashews, pistachios, and macadamia nuts I like them too. The ones that taste the worst for me are Brazil nuts.
Lepidium meyenii, known as maca or Peruvian ginseng:
I happen to have had a bag of gelatinized maca powder for some time. I didn’t remember it was there, but cleaning up I moved them around, and today I was cooking when the smell hit me. I immediately felt an urge to eat it (I mix it with coconut cream and strawberries). It tasted delicious–which was surprising to me, as maca has a peculiar taste that borders on the unpleasant (earthy and ashy) and I have not given it as many opportunities to develop an acquired taste.
Best,
Hector
That’s helpful. I’m eating the snack size sheets. 😆 Ex. SeaSnax and gimMe. This translates to around 5g of these, which is 10 small sheets.
I’m going to switch to the large sheets since those will be more versatile. That’s wonderful that you found a local source of duck eggs.
Hi,
I am sharing a little more of my experiences on the food-only approach.
…
My highest-reward food has become runny duck egg yolks and nori seaweed. More so if I eat them together, as awkward as that may be!
…
With nori seaweed I have several funny stories. Visiting relatives have tried it, and it hasn’t had many compliments: “it tastes like fish” and “it tastes like what turtle food smells like”. Someone turned red and almost vomited, oops.
Curious how taste is that subjective. To me, nori seaweed doesn’t taste like that at all. It certainly has a strange taste, which I think they call “umami”, but it also has a toasted flavor, even slightly nutty –delicious overall.
Before developing any craving one must first overcome the “acquired taste barrier” for those foods that are not part of our culture (such as liver or seaweed). But in my case, I didn’t have to do anything in this regard. The first bite I ever had did taste like sardines. But only the very first bite. The rest was good to me, and practically the next day I began to love it.
(By the way, I don’t think the “sardine flavor” is a good thing. I’ve seasoned frying pans with flaxseed oil –very rich in vegetable omega 3– and you have to burn it in order to make it undergo polymerization and cover the stainless-steel pores. It turns out burned flaxseed oil smells exactly like grilled sardines, so we can assume the smell comes from omega 3 being damaged or becoming rancid.)
…
Regarding nori brands, I said I was buying this: https://www.amazon.es/gp/product/B07VHD8MVY/ref=ppx_yo_dt_b_asin_title_o01_s00?ie=UTF8&psc=1
But I recently bought this one: https://www.amazon.es/gp/product/B0933TD61V/ref=ppx_yo_dt_b_asin_title_o01_s01?ie=UTF8&psc=1
Both are good. The first one is crispier, but tastes unreasonably much better to me – i.e., both are almost indistinguishable, but for any reason I clearly prefer the first. By the way, based on my body temperature, I would say the second has more iodine; based on the label, about 130 mcg per sheet (they say 0,2 mg per 1 sheet and half).
…
Regarding coconut milk and macadamia nuts, I had said I preferred the first. But not anymore. It turns out coconut milk was delicious because it was combined with other food (in the same way butter turns delicious when it is spread in a potato with a bit of salt). I am now bored with coconut milk and much prefer macadamia nuts. By the way, I tried three different brands of macadamia nuts, and there is a huge difference between how good they taste, so be careful when buying them! And raw (vs. toasted and highly salted) taste better to me.
…
Finally, I can’t comment much on other foods as I have not yet been able to implement the complete food-only approach. The cause is that I have been suffering from dysbiosis for months, which causes chronic diarrhea and FODMAP intolerance. This has nothing to do with the food-only approach, as it started long time before any dietary change. I am emphasizing intermittent fasting; following circadian rhythms; eating egg yolks; taking vinegar; taking vitamin C (supplement); taking taurine in the morning (supplement); taking extracellular matter broths in the afternoon; optimizing vitamin A and D; and optimizing copper and zinc. When I solve this problem, I will do a bit more structured (but subjetive after all) experiments, and blood tests.
Best,
Hector
A little update:
I’ve decided I will double either the number of macadamia nuts –I buy them in 125 g packets– or the amount of coconut milk –I buy it in bricks of 1 L with 18% fat– to increase dietary fat; and I would add 250 g of fresh mushrooms to the 1 kg of frozen mixed mushrooms in order to further increase the B-vitamins.
See the new balance of nutrients here:
https://i.imgur.com/QkSNmt3.png
I think it looks good!
Two concerns I have yet to research:
— Fungi are enormous living beings that theoretically can occupy kilometers of surface under the ground (the mushrooms are their reproductive organ). So I imagine that cultivated ones are perhaps less nutritious, but safer in terms of heavy metals. Many frozen mushrooms come from China, so you have to be sure to get frozen local mushrooms.
— I’m not sure how healthy coconut milk is. The ingredients from mine are 75% extract from coconut, and water. This seems to be emulsified. If I recall correctly, coconut has some special protein that can produce an emulsification naturally. When stored in the fridge, it becomes thick as whipped cream. It’s delicious. But I’m not aware of how it is produced (I think that coconuts are simply grated) and if it alters the product in a harmful way (e.g. the homogenization process for milk is pretty simple, yet it might introduce pernicious effects due to the breakage of the milk fat globule membrane; see: http://perfecthealthdiet.com/q-a/comment-page-84/#comment-1869203).
Best,
Hector
“In short, the optimal macronutrient proportions for building muscle are to eat carbs at the natural carb intake— about 30 percent of calories— and protein and fat in the proportions found in the body as a whole— thus, splitting the remaining calories 74 percent as fat and 26 percent as protein. That works out to a 30 percent carbs, 18 percent protein, 52 percent fat diet.” -p138
Wait, so are you saying there’s 3x as much fat as protein in muscle (26 * 3 = ~74)? I’ve never heard that anywhere else.
He says, “in the body as a whole.” Unless there is a part you didn’t post, it isn’t saying what you think.
Hi tamahome02000,
Fat has more than double the energy density of protein. 1 g of fat is 9 calories, while 1 g protein is only 4.
26 % of calories derived from protein equals 26/4 = 6,5 g of protein per 100 g
74 % of calories derived from fat equals 74/9 = 8,22 g of fat
You can see that muscle cointains about the same proportion in mass of fat and protein, but about 3/4 of fat and 1/4 of protein if you talk in terms of calories. Of course these proportions will actually vary depending on the cut of meat and on the leanness.
Best,
Hector
What is your opinion on buckwheat and quinoa on this food plate? I eat those as my primary carb sources and was considering sprouting them too
Hi Drake
If you use the search function on the site you can find the answers to these types of questions.
Paul has said in the past that buckwheat is ok – in fact I think that question came up again just recently.
As for quinoa, here’s what he says:
http://perfecthealthdiet.com/page/125/
Best
Peter
Thank you!
http://perfecthealthdiet.com/the-diet/comment-page-30/#comment-1879302
Hi Eric,
I’m a bit confused by your affirmation that “lithium, silicon, and boron [are good candidates to be supplemented] because the main source is not diet, it is […] drinking water”. From: https://perfecthealthdiet.com/the-diet/comment-page-30/#comment-1883817
From eyeballing this study, which includes many foods, https://www.sciencedirect.com/science/article/abs/pii/S0278691513007011?via%3Dihub, it seems like the concentration of lithium in most foods is not insignificant. Nuts contain the most: 8.761 ± 5.368 mg/kg — in my case, as I eat about 30-40 g per day, that would account for 0,30 mg of lithium. But most of the other foods contain in the order of 2 mg/kg. For this population, the daily intake of lithium per day was estimated to be 3,674 mg. In comparison, Paul recommends –optionally– 1 mg of lithium from supplements per day. And waters rich in lithium contain 1 to 2 mg of lithium per L. Are we sure that we really need to get some lithium from water or supplements in order to optimize it? Because looking at these figures, it doesn’t appear that water is a much better source (although of course I don’t doubt it may be helpful if we want to optimize the intake of every nutrient in the diet, as water offers minerals with no calories). What do you think?
Now, with regard to boron, I recall you said that boron could be optimized by eating, I believe, 5 avocados per week (I suppose the small ones, the Hass variety). Have you changed your mind?
And, with regard to silicon, I still haven’t explored it.
…
In making these questions, a bit more context would have been helpful. Therefore, if you got the time, I’ve a few more questions:
1. What amount of silicon, lithium and boron are you personally aiming for? (Paul recommends –as optional supplements– 1 mg of lithium per day; up to 25 mg of silicon per day; and a 3 mg supplement of boron 1-3 times per week).
2. In case that you are supplementing those instead of getting them from water, what forms have you chosen? (Typically, lithium seems to be available as orotate or aspartate, and as ionic forms (if I recall correctly, the ionic form is mostly used for psychiatric diseases and may be less desirable for some reason – I would need to re-check this). Boron, as boric acid, boron citrate, -aspartate, or -glycinate. Silicon, from orthosilicic acid, or natural sources such as Lithothamnion Corallioides, or horsetail extracts).
3. By the way, I have trouble to learn about silicon in water. The problem is, the studies of water composition that I found show the concentration of silica (SiO2). Silica contains 46.69 percent silicon by weight, but I don’t expect silicon in silica to be bioavailable as it is an oxide difficult to ionize. But even if it were bioavailable, we could just eat a bit of sand every day :-). So, there must be many compounds that are of our interest, and SiO2 isn’t one of them. A quick search says that silicon is present as ortho silicic acid (H4SiO4, or Si(OH)4), which is a product of the solubilization of SiO2. This also suggest volcanic waters are richer in silicon; see: https://www.lenntech.com/periodic/water/silicon/silicon-and-water.htm. So, do you know how I should interpret the data in these studies? If the SiO2 data were not useful for our purposes, then I wonder how can I find the concentration of silicon for a given water, as this figure doesn’t appear in the tables I looked at.
…
Some other comments that may be of interest for Europeans:
— I tried to find Rozana water from Auvergne, France –not to confuse with Roxane brand, which is from USA— but it seems impossible to find in Spain. (Eric said about 1/3 L of this water would optimize the intake of boron, lithium, and silicon – really great).
— Then, I noticed that there is another brand of water from Auvergne: Volvic, owned by Danone, much easier to find internationally. See: https://en.wikipedia.org/wiki/Volvic_(mineral_water). But by looking at its composition it is obvious that it is completely different from Rozana and much lower in minerals; see: https://www.volvic.co.uk/volcanic-water/composition.
— So, I continued my search. This seems like the best source to check the composition of European bottler waters, but I’ve been unable to access it: https://www.schweizerbart.de/publications/detail/isbn/9783443010676/Geochemistry-of-European-Bottled-Water
So, by looking at individual studies, it looks like there are some interesting local options. E.g., when searching for waters rich in lithium, in Portugal there are some good options. The brands are: Vidago (2210 mcg of Li+ per L), Bem-Saúde (2000), Pedras Salgadas (1800), Frize (1760) and Campilho (1590). Source: https://pubmed.ncbi.nlm.nih.gov/33198207/. But so far these brands seem to be surprisingly difficult to find out of Portugal, even in Spain. For Spaniards reading this: at least Pedras Salgadas may be found in some supermarkets in Spain, see: https://soysuper.com/search?q=pedras+salgadas – and its composition can be found here: http://finewaters.com/bottled-waters-of-the-world/portugal/pedras. Also in Spain, Vichy Catalán is said to be high in lithium (1,2 mg per L) and silicon (I don’t know how much though) — but it’s pretty rich in sodium and I prefer to have sodium on my food rather than drinking it.
I will post any useful results I find in the future.
Best,
Hector
Hi Hector,
Thank you, you make very interesting points. One caution, the first study is from the Canary Islands and a volcanic island may be an unrepresentative source, since volcanoes are a primary source of most available lithium. (E.g., https://teen.wng.org/node/3310, “Most [lithium] comes from the rocks and groundwater near volcanoes.”) So food grown in the Canary Islands would be unusually lithium rich. How much of the food in the study originated from the Canary Islands, I don’t know.
Best, Paul
Thank you, Paul — you’re totally right. Out of curiosity, will it also apply for boron? Rozana water is volcanic and very high in both lithium, silicon, *and* boron.
In fact, in the table in that study, one column shows the origin of the samples. I should have looked at it a bit more; I was underestimating the islands’ ability to self-supply, but almost all the foods tested were from the Islands. Then, finally, reading a bit more, in page 865, it shows lithium intake for other populations: Belgica (0.0086 mg Li+), UK (0.016), France (0.011), and Vietnam (0.03626)… Compare that to 3.674 in Canary Islands.
Sorry for not reading enough! Now, a vacation to replenish our lithium deposits, anyone?
Hi Hector,
Mineral water will contain Boron as orthoboric acid (B(OH)_3), Silicon as orthosilicic acid (Si(OH)_4), and Lithium in free ionic form (Li+). These are the forms of these nutrients that would have supplied most of the intake throughout most of human evolution, and for which we have the best evidence of benefits.
Many foods have silicon, almost none of it as orthosilicic acid. The bioavailability of the silicon species found in most foods is approximately zero.
On paper avocados have plenty of Boron. But I don’t think it’s present as orthoboric acid.
For Rozana, 1/3 liter would supply about 14 mg silicon, 220 mcg boron, and 750 mcg lithium. I think these are sensible amounts.
I emailed you some data that you might enjoy.
Best,
-Eric
Thank you, Eric. That is incredibly useful. After gaining two diopters, I can say that this is the best water I have found in supermarkets in Spain (for which I have data, surely).
CABREIROÁ MAGMA is high in boron and lithium; and moderate in silicon; so, by drinking two liters a week you probably optimize the intake of boron and lithium and provide a good amount of silicon.
However, if one is picky and wants more silicon, then:
FUENTE ALTA (Tenerife water) is high in silicon, but low in boron and lithium (compared to magmatic waters, not compared with tap or most waters), so if you take one liter a week, along with the two liters a week of CABREIROÁ MAGMA, you may optimize silicon as well.
…
IN TOTAL, combining both waters (2 L of CABREIROÁ MAGMA per week plus 1 L of FUENTE ALTA per week), you would be averaging:
560 mcg of boron, 650 mg of lithium, and 14 mcg of silicon per day.
(If you instead take 1,5 L of FUENTE ALTA per week –as you may find it in 1,5 L bottles–, then you get 18 mcg of silicon.)
IF you only take CABREIROÁ MAGMA, then:
Idem boron and lithium, but 7 mcg of silicon instead of 14 mcg.
…
Regarding the price for Spaniards:
FUENTE ALTA costs 0,16€ if bought in 8 L bottles or 0,26€ in 1,5 L bottles. (But I couldn’t find it; maybe that price is for Canary Islands only.)
CABREIROÁ MAGMA costs around 1€ per L (you may find it in Alcampo or Supercor). (Be careful, Cabreiroá sells another type of water that is not magmatic and does not contain these minerals.)
By the way, FUENTE ALTA also contains a bit of vanadium: 7 mcg/L.
Best,
Hector
Hi Paul
in the book, Carbohydrates chapter, “Glucose for Muscle Glycogen”, there are the energy expenditure for various form of exercise, but there is not resistance training among them. What do you think would be the tot caloric expenditure for a 160lb man during resistance training?
I found this calculator, and 60min of resistance training for a 160lb man is 419cal, would you agree with the calculator?
https://caloriesburnedhq.com/calories-burned-weight-lifting/
Hi Paul,
You should post this interview to your site: https://wellnessmama.com/podcast/490/. This guy really knows his stuff! 😀
Just read about farro? What do we think of it?
Dear Paul,
What would you buy for your emergency food supply?
Thanks,
Rose